Golden Era of Self-Cell Repair
Tony had tried pretty much everything that conventional medicine had to offer. He had also given natural solutions such as supplements, hormones, and diet changes a shot as well, yet he was still in pain. Tony was facing multiple joint replacements and surgeries. A new law, the Federal Right to Try Act of 2017, empowered Tony to try a new option. His 18-month patient-reported outcome is remarkable. As he reported, “To be candid, the difference in the quality of my life is just unbelievable. You can’t describe to someone what it is like to live without that ever-present and often excruciating pain.” Is a Golden Era of Healthcare within our grasp?
Many millions of people live with (and die because of) poor health despite treatment with surgery, drugs, and devices (the standard of care). Doctors refer to these patients as “no-option.” They are considered resistant to treatment. Put simply, the standard of care isn’t working well – if at all – for no-option patients. Some get relief from natural solutions such as diets, supplements, and the like (integrative medicine). But many, including Tony, also fail to achieve sustained benefit from those.
In 1991, Arnold Caplan, Ph.D., in his foundational paper, Mesenchymal Stem Cells. created a vision “for the emergence of a new therapeutic technology of ‘self-cell repair’ (emphasis added).” With that, Dr. Caplan conceived of a new standard of care for no-option patients like Tony and set the foundation for a Golden Era of Healthcare.
We will dig into what Self-Cell Repair means and how the science has evolved since Dr. Caplan first presented its potential. We will also share Tony’s full patient-reported outcome. And fill in the blanks on the Right to Try Act of 2017.
Healthcare’s Gordian Knot
The term “Gordian knot” is commonly used to represent an unsolvable problem. A Roman historian described it as “several knots all so tightly entangled that it was impossible to see how they were fastened.” The name traces back to a legendary event where Alexander the Great used his wit and cunning to cut the Gordian Knot.
 Alexander’s feat is trivial compared to untying the intricate web of tangles involved in caring for no-option patients. This dilemma is even more complicated than it may first appear.
Alexander’s feat is trivial compared to untying the intricate web of tangles involved in caring for no-option patients. This dilemma is even more complicated than it may first appear.
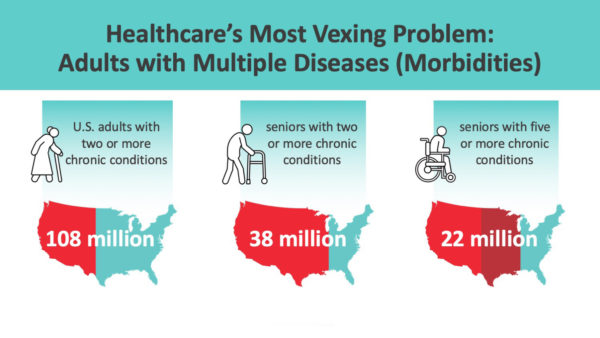
- Over 100 million American adults are living with two or more chronic illnesses (co-morbidities).
- For seniors, it is even more daunting: 68% (38 million) have two or more, and 40% (22 million) have five or more chronic conditions, respectively.
- On average, those 65 and over go to seven doctors and take seven meds per year.[1]
Epic Failure of Conventional Medicine
All of us know someone who is living with one or more chronic conditions:
- Perhaps a friend had back surgery, and two years later, they are back in the soup with disabling pain. There are more than 4 million patients with “failed back” (surgery) syndrome.
- Or, a family member has both heart disease and diabetes. Over 10 million people in the U.S. have this life-threatening combination.
- More than 2 million patients in the U.S. have both rheumatoid arthritis and psoriasis. R.A. involves inflamed and painful joints. Psoriasis is a skin disease. The combination of the two is so prevalent it has morphed into one diagnosis, psoriatic arthritis.
- Over 20 million Americans live with incurable neuropathies (nerve pain or numbness).
Our reliance on conventional medicine is rooted in thousands of years of development and practice. Corporations, investors, government agencies, and research institutions invest hundreds of billions per year to improve the standard of care. Yet, as the stats above tell us, the number of people living with one or more chronic diseases has become a crisis of magnitude.
- The conventional drugs used to treat long-term maladies such as rheumatoid arthritis (R.A.), Parkinson’s Disease, heart disease, and diabetes cost between $25,000 – $50,000 (or more) per year.
- Worse, these meds do not cure the prescribed for conditions – and they often come with intolerable side effects. For too many ill people, “the cure is worse than the disease”;
- Hence, many patients discontinue use or refuse to take their prescribed drugs—non-compliance then piles on even more cost.
Despite the costs and risks, big pharma makes tens of billions off of their blockbuster drugs. And, they unapologetically raise prices 10% a year in and year out.
Tony was just one of the millions of patients in search of a new standard of care.
What is Self-Cell Repair?
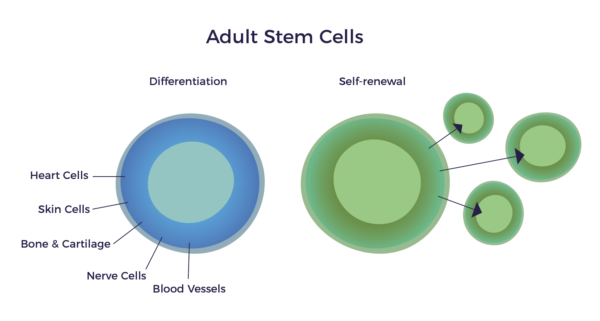
Returning to Dr. Caplan’s 1991 paper, Mesenchymal Stem Cells, he described MSCs as adult stem cells. He explained that MSCs could change into (differentiate) into multiple tissue types as well as neurons and blood vessels and self-renew. In other words, he hypothesized that MSCs would grow of new heart muscle, cartilage, nerves, or blood vessels in man.
A Surprising Discovery
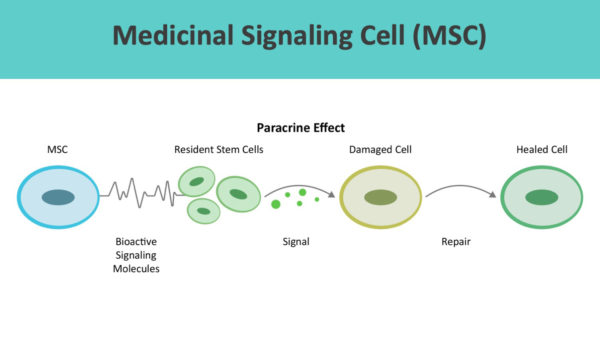
In an unexpected twist, Dr. Caplan proposed to change the name of MSCs to Medicinal Signaling Cells in 2010. He wants to drop the reference to stem cells altogether.[2] To paraphrase his thinking, MSCs release hundreds of beneficial signaling molecules called cytokines. These cytokines tell the resident stem cells at the site of injury or disease to do their jobs. As it turns out, the benefits of MSCs come from what the cytokines do rather than what the MSCs become.
In other words, we have our own personalized “pharmacy” that knows how our body and its systems work. When there is something abnormal or out of balance, the cytokines go to where they are needed – sites of inflammation. They then signal the resident stem cells to get to work and set it right. This nearby cell-to-cell communication is called the paracrine effect.
 As a testament to Dr. Caplan’s vision and research, according to a PubMed search, there are over 150,000 published papers that discuss MSCs and 1,000 trials registered on Clinicaltrials.gov, respectively.
As a testament to Dr. Caplan’s vision and research, according to a PubMed search, there are over 150,000 published papers that discuss MSCs and 1,000 trials registered on Clinicaltrials.gov, respectively.
What does fat have to do with all that?
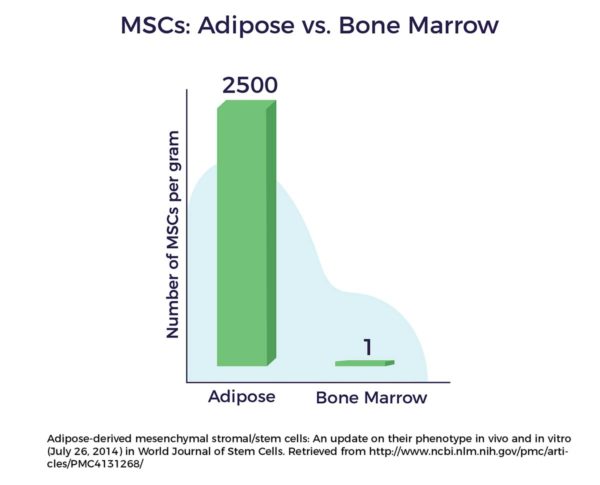
The game-changing breakthrough came in 2001 when Patricia Zuk Ph.D. and others, working in the labs of UCLA, discovered MSCs residing in our fat.[3] And that adipose-derived MSCs were more accessible, abundant, and potent than those from the bone marrow.
Dr. Zuk’s finding advanced a prior discovery: In the 1960s, a Nobel Prize winner, Martin Rodbell, had isolated a population of regenerative cells in our fatty tissue.
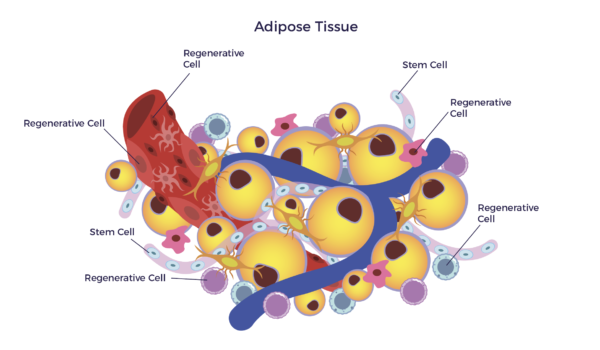 In other words, there is a mixed population of stem cells and other regenerative cells in our fat. When clinical grade, this diverse mix of cells are called Adipose-Derived Regenerative Cells (ADRCs).
In other words, there is a mixed population of stem cells and other regenerative cells in our fat. When clinical grade, this diverse mix of cells are called Adipose-Derived Regenerative Cells (ADRCs).
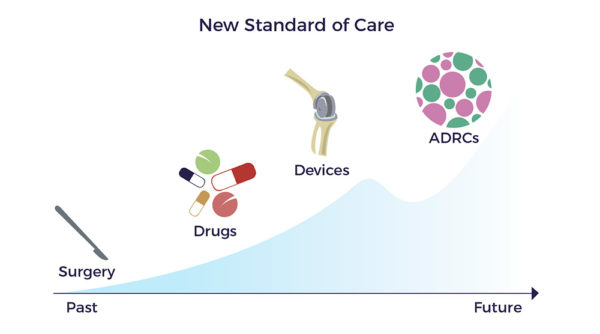
Dr. Caplan’s, Dr. Rodbell’s, and Dr. Zuk’s breakthroughs are the foundation for a new standard of care and a Golden Era of Healthcare.
The Gold Standard for Judging Outcomes for Patients like Tony?
Magnetic resonance imaging (MRI) is a test that uses powerful magnets, radio waves, and a computer to make detailed images of the inside of your body. Doctors use MRIs to diagnose everything from the brain to the heart and other organs, as well as your spine and joints. They also use these tests to see how well you’ve responded to treatment.
While MRIs are considered the gold standard for diagnostic imaging, there is a problem with relying solely on their findings. That is because a patient’s symptoms and dysfunction often do not correlate with their structural abnormalities. As but one of many possible examples, patients with significant back pain can have MRIs that are not so bad, yet they are more symptomatic than those with imaging that shows severe signs of degeneration.
The medical establishment relies on MRIs and other diagnostic tests to establish objective evidence that surgery or other treatment worked. In contrast, patients care about their quality of life.

As Tony put it:
What is the “Right to Try”?
“Right to Try” is a new way to express our fundamental “right to life” and “right to health.”
On May 30, 2018, an enlightened and extraordinarily humanitarian bill, The Federal Trickett Wendler, Frank Mongiello, Jordan McLinn, and Matthew Bellina Right to Try Act of 2017 (Right to Try Act), was signed into law by President Trump. [4] [5] The law provides patients who are seeking new treatment options not approved by the FDA the right and opportunity to do so. The law empowers no-option patients to take control of their health.
Importantly, not all patients with chronic disease meet the criteria. The patient and their doctor determine eligibility under the law.
Golden Era of Healthcare
The great monuments, art, philosophy, architecture, and literature of the Golden Age of Greece (500 BC – 300 BC) are the building blocks of western civilization.
The architects of self-repair cell therapies and the Federal Right to Try Act provide the building blocks for a Golden Era of Healthcare – and a new standard of care for patients like Tony.
To find out whether you might qualify for AMBROSE Cell Therapy under the Right to Try law, please click here.
To read more about AMBROSE Cell Therapy patient-reported outcomes, including Tony’s, please click here.
[1] http://www.webmd.com/healthy-aging/features/how-many-drugs-are-you-taking#1
[2] A Caplan Mesenchymal Stem Cells: Time to Change the Name! Stem Cells Translational Medicine 2017;6:1445–1451
[3] PA Zuk et al Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng 2001
[4] https://www.congress.gov/115/bills/s204/BILLS-115s204enr.pdf