¿Se puede hacer algo por los Covid Long-Haulers?
¿Se puede hacer algo por los Covid Long-Haulers?
Después de vivir con graves síntomas de covaginitis prolongada y problemas de salud preexistentes, Brian ejerció su derecho a probar la terapia celular AMBROSE en noviembre de 2021. Dice que AMBROSE ha tenido "un efecto enorme en mi salud y calidad de vida". Brian añade que, nueve meses después, "estoy haciendo cosas que no podía hacer hace un mes".
Sorprendentemente, los numerosos beneficios de Brian se produjeron a pesar de las continuas tensiones empresariales y la difícil pérdida de dos familiares.
Fondo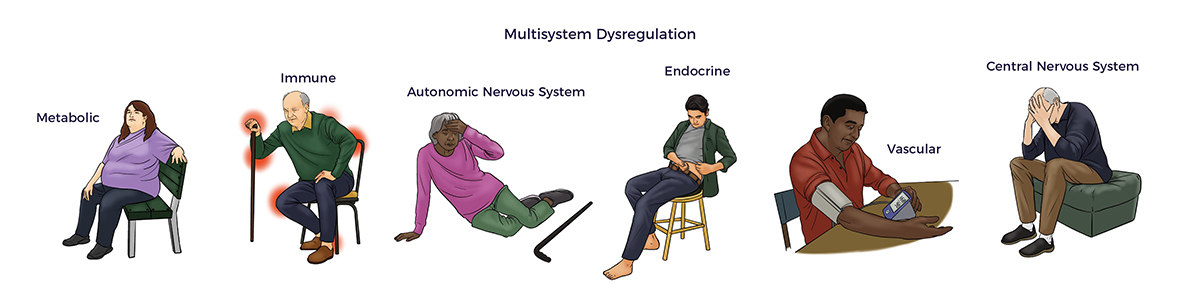 Desde diciembre de 2019, el coronavirus 2 del SRAS (SARS-CoV-2) se ha extendido como la pólvora por todo el mundo. A diferencia de la gripe estacional o el resfriado, el COVID-19 puede atacar todos los sistemas corporales y múltiples órganos.
Desde diciembre de 2019, el coronavirus 2 del SRAS (SARS-CoV-2) se ha extendido como la pólvora por todo el mundo. A diferencia de la gripe estacional o el resfriado, el COVID-19 puede atacar todos los sistemas corporales y múltiples órganos.
En respuesta a las capacidades de tierra quemada del virus, investigadores de células madre de todo el mundo han colaborado para mejorar los resultados de los pacientes de alto riesgo de Covid y de los de largo recorrido. [1]
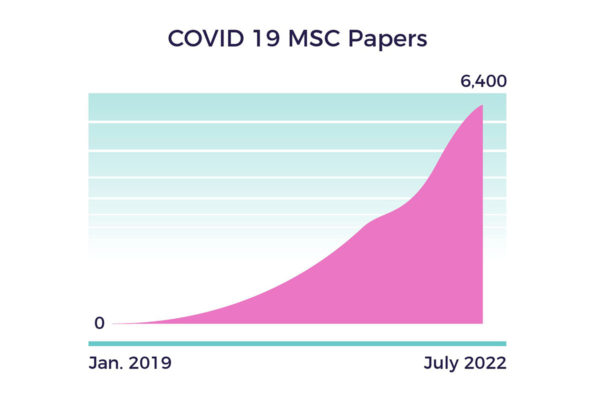
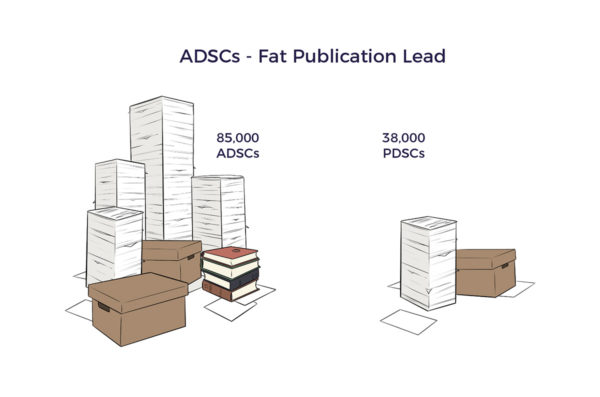
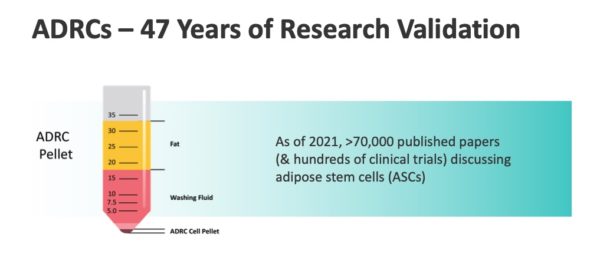
Los investigadores se basaron en más de 200.000 artículos publicados sobre células madre mesenquimales (MSC). En julio de 2022, su urgencia se tradujo en 6.400 artículos o unos 12 diarios.
 Los estudios de MSC en humanos incluyeron las inducidas por Covid:
Los estudios de MSC en humanos incluyeron las inducidas por Covid:
- Síndrome de dificultad respiratoria aguda (SDRA) [2]
- Síndrome inflamatorio multisistémico en niños [3]
- Enfermedad multiorgánica, incluida la parada cardiaca súbita [4]
- COVID-19 neumonía en abril de 2020. [5]
El Dr. Pietro Gentile y otros centraron sus investigaciones en las células madre derivadas del tejido adiposo (ADSC) y las ADRC. [6] [7] [8] [9]
¿Pueden los ADRC ayudar a los usuarios de Covid de larga distancia?
 Lo más prometedor para Brian es que sus síntomas de Covid se entrecruzaban con los de la hipermovilidad, las conmociones cerebrales, la insuficiencia renal, la enfermedad de Lyme y los efectos secundarios de la quimioterapia.
Lo más prometedor para Brian es que sus síntomas de Covid se entrecruzaban con los de la hipermovilidad, las conmociones cerebrales, la insuficiencia renal, la enfermedad de Lyme y los efectos secundarios de la quimioterapia.
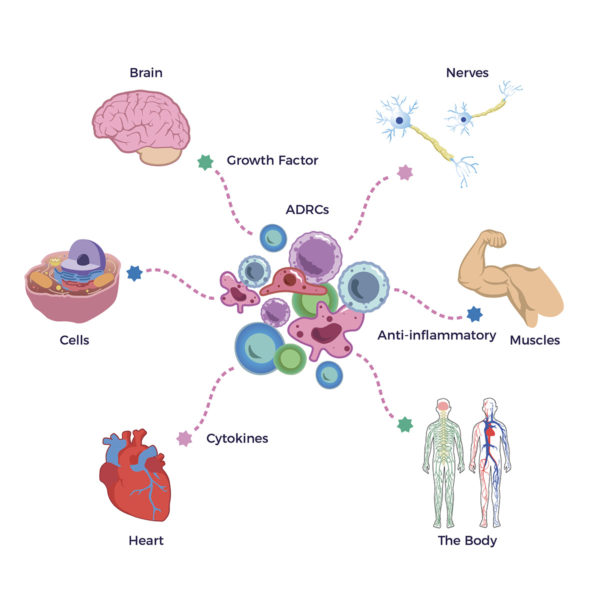
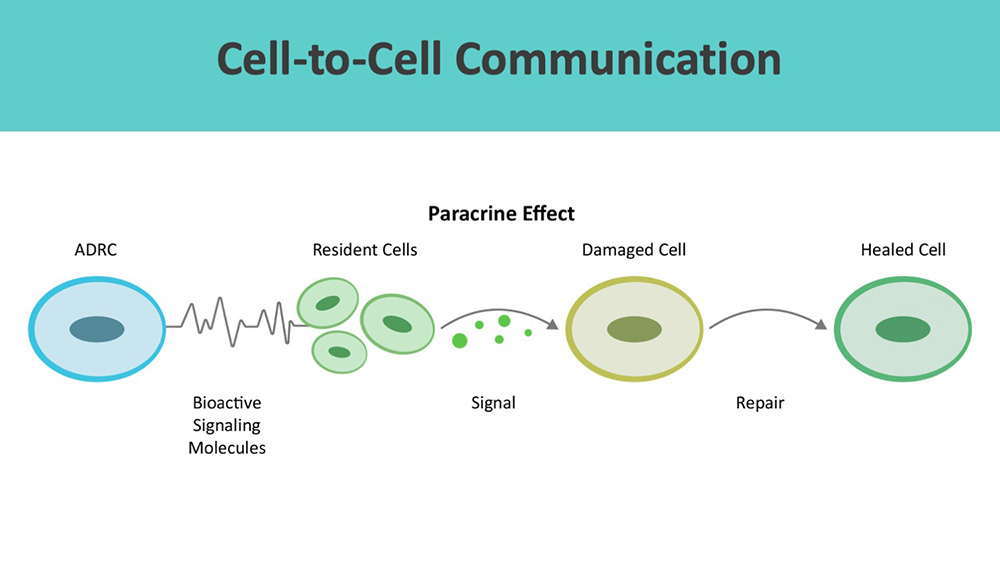
En respuesta a una o varias de estas agresiones, nuestros ADRC segregan factores de crecimiento (GF) y proteínas de señalización antiinflamatoria o citoquinas esenciales para nuestro cerebro, corazón, músculos, nervios, células y salud corporal en general.
Compartimos más sobre los GF y las citocinas en la historia de Brian que sigue.
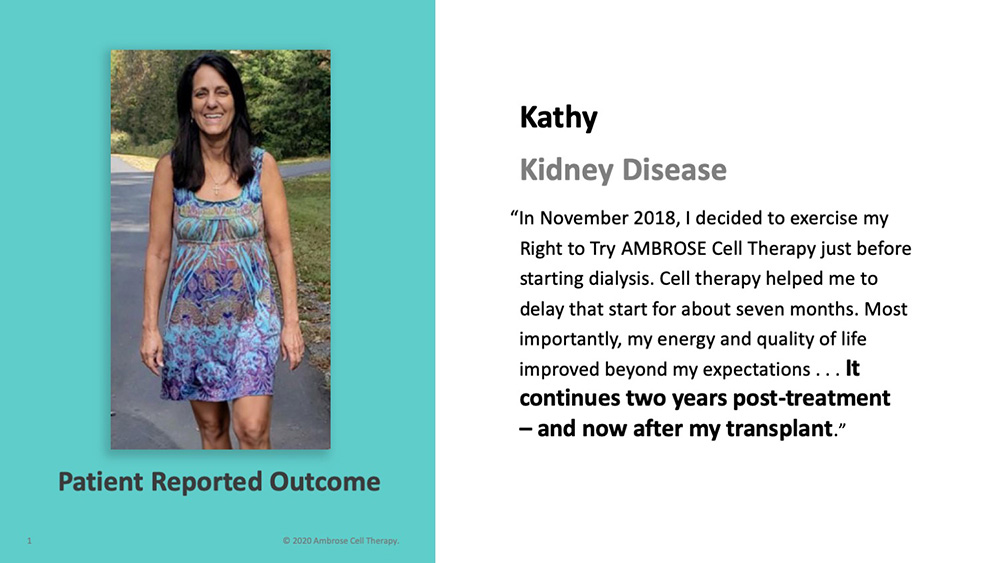
Pacientes de Ambrose Trish, Wouter, Kathy, y otros pacientes con niebla cerebral, fatiga, dolor articular, etc. respondieron a la terapia basada en ADRC. Por lo tanto, para Brian tenía sentido probar la terapia celular AMBROSE.
La historia de Brian
En diciembre de 2020, el médico de Brian lo ingresó en la UCI del Cedar-Sinaí con COVID-19, y volvió a casa como paciente de larga estancia de Covid al cabo de dos semanas.
Tras una llamada introductoria con Matt Feshbach, Consejero Delegado, AMBROSE le proporcionó una consulta médica educativa, artículos de información general y documentos revisados por expertos que respaldan la seguridad y la eficacia potencial de la terapia para el covídrio largo y las demás afecciones que le afectan. Brian dijo: "(Matt) respondió a mis preguntas. Comprendí lo suficiente como para seguir adelante".
Covid Long-Hauler Síntomas Brian experimentó los síntomas clásicos de la enfermedad de larga duración: niebla cerebral, fatiga crónica y volatilidad emocional. Como él mismo resumió: "La mayor parte de 2021 fue un año perdido".
Brian experimentó los síntomas clásicos de la enfermedad de larga duración: niebla cerebral, fatiga crónica y volatilidad emocional. Como él mismo resumió: "La mayor parte de 2021 fue un año perdido".
Empezó a notar los beneficios poco después de su tratamiento con AMBROSE. "Al cabo de un mes, noté una enorme mejora en mi claridad mental y mi energía. Mis compañeros de trabajo también notaron la diferencia. No me di cuenta de la gravedad de la fatiga hasta que recuperé las fuerzas".
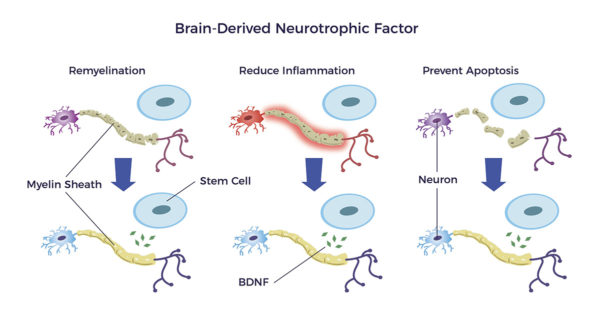
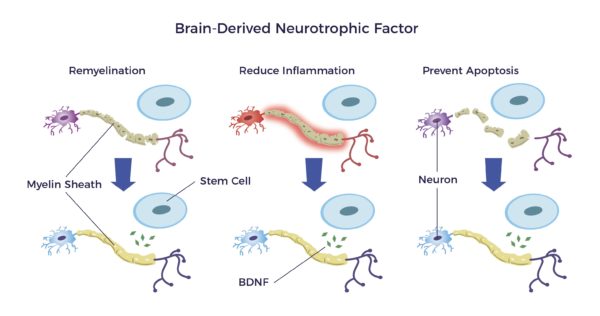
 Apoyando las declaraciones de Brian, los ADRC publican "Factores neurotróficos (NTFs),” Neuro relativa a los nervios y tróficadel griego antiguo trophikósque significa "de alimento o nutritivo". Los NTF, a través de múltiples mecanismos, reducen la neuroinflamación y estimulan el desarrollo de nuevas células cerebrales, conexiones de células cerebrales y nervios. [10] [11]
Apoyando las declaraciones de Brian, los ADRC publican "Factores neurotróficos (NTFs),” Neuro relativa a los nervios y tróficadel griego antiguo trophikósque significa "de alimento o nutritivo". Los NTF, a través de múltiples mecanismos, reducen la neuroinflamación y estimulan el desarrollo de nuevas células cerebrales, conexiones de células cerebrales y nervios. [10] [11]
Al igual que los fertilizantes mantienen las plantas sanas y en crecimiento, los factores neurotróficos actúan como Miracle Grow para el cerebro.
El restablecimiento de la energía y la claridad mental de Brian tienen sentido a la luz de lo anterior.
Vasculitis Covid dejó a Brian con una inflamación debilitante de los vasos sanguíneos y una hinchazón en ambas piernas, o vasculitis, una enfermedad autoinmune. También se quejaba de entumecimiento y hormigueo constantes en ambas piernas (neuropatía). La pierna derecha era peor que la izquierda.
Covid dejó a Brian con una inflamación debilitante de los vasos sanguíneos y una hinchazón en ambas piernas, o vasculitis, una enfermedad autoinmune. También se quejaba de entumecimiento y hormigueo constantes en ambas piernas (neuropatía). La pierna derecha era peor que la izquierda.
"Mi vasculitis y neuropatía desaparecieron poco después del tratamiento".
Además de los NTF, los ADRC segregan factor de crecimiento endotelial vascular (VEGF). El VEGF mejora la circulación, reduce la inflamación y estimula el crecimiento de nuevos vasos sanguíneos.
También en este caso tiene sentido que los vasos sanguíneos y los nervios inflamados de Brian se calmaran. Y una gran cantidad de literatura apoya la experiencia subjetiva de Brian. [12] [13]
Y volvamos al cerebro de Brian: El VEGF reduce la neuroinflamación y mejora el flujo sanguíneo en el cerebro. Por el contrario, la neuroinflamación y la falta de flujo sanguíneo en el cerebro causan fatiga crónica, niebla cerebral y problemas de memoria. [14] [15]
Condiciones preexistentes
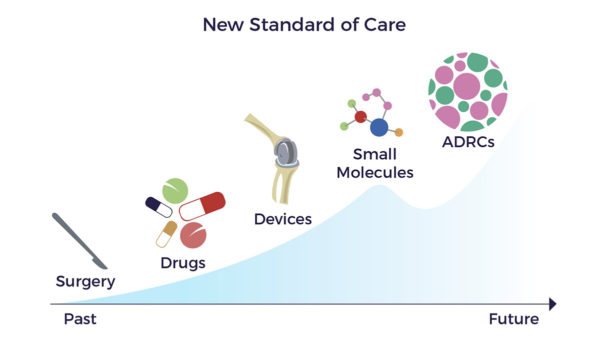
Brian ingresó en el hospital con una galaxia de dolencias preexistentes que no habían mejorado con cirugías, fármacos y dispositivos.
Antes de la pandemia, Brian vivía con:
- Obesidad
- Artritis en la parte baja de la espalda, hombros, caderas y rodillas.
- Asma
- Fractura de costillas
- Osteopenia (una fase temprana de la osteoporosis) y
- Un leve agrandamiento del corazón y dificultad para respirar
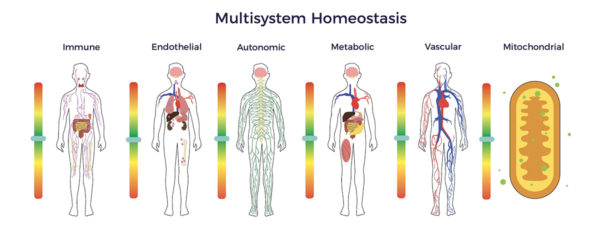
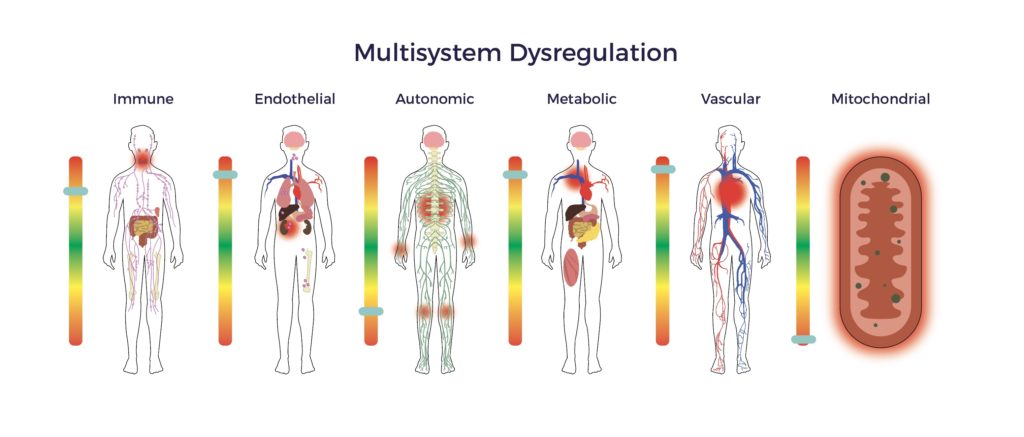
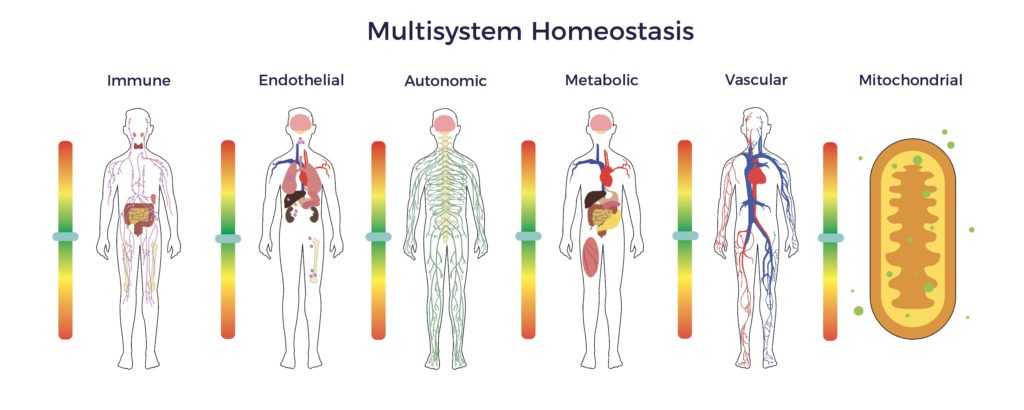
En resumen, Brian sufría una desregulación multisistémica.
Sus medicamentos incluían Prednisona 30 mg diarios, Singulair, Symbicort y Spiriva para el asma. Ambien para dormir.
¿Pueden los ADRC ayudar a las personas de larga distancia de Covid con enfermedades preexistentes?
En 2016, el Instituto de Medicina Regenerativa de California (CIRM) contribuyó a la financiación de dos artículos de revisión que apoyaban el tratamiento basado en ADRC para las enfermedades crónicas de Brian. Además, investigadores preeminentes de la Universidad de Tulane y otras instituciones de investigación respetadas han continuado el creciente apoyo al potencial de los ADRC para tratar múltiples enfermedades. [16] [17] [18]
Obesidad
Brian ha luchado con su peso desde muy joven. "Probablemente he perdido 136 kilos a lo largo de mi vida. Probé la cirugía bariátrica en 2007, pero recuperé el peso".
"Desde mi tratamiento, he bajado unos 15 kilos y he mantenido mi peso dentro de un rango inferior con una dieta menos restrictiva por primera vez".
En 1994, el superdetective Jeffrey M. Friedman, de la Universidad Rockefeller, estableció que la grasa es un órgano endocrino. En pocas palabras, descubrió que las células adiposas segregan hormonas que regulan el aumento de peso. Su descubrimiento explica la mejora del metabolismo y la quema de grasa de Brian tras su tratamiento de terapia celular. [19] [20]
Desgaste y traumatismos
Brian jugó al fútbol en el instituto, lo que le provocó algunos traumatismos craneoencefálicos. A los 20 años sufrió varios accidentes de tráfico graves. Quedó inconsciente dos veces. "Me llevaron al hospital varias veces; fue bastante grave".
El fútbol, el baloncesto, el béisbol, el esquí y el exceso de peso tampoco fueron benévolos con las articulaciones de Brian.
- Tres operaciones de la rodilla derecha fracasaron, dejando ambas rodillas doloridas.
- Sufría artritis degenerativa en los hombros.
- También tenía artritis en las caderas derecha e izquierda.
Las inyecciones de esteroides en las articulaciones afectadas no consiguieron aliviar a Brian. Probó con inyecciones de células madre de médula ósea en los hombros, pero eso "no funcionó en absoluto".
El especialista en dolor intervencionista de Ambrose desarrolló un plan de tratamiento personalizado basado en un Protocolo maestro. Aplicó 22 inyecciones de grasa micronizada enriquecida con PRP en las doloridas articulaciones de Brian.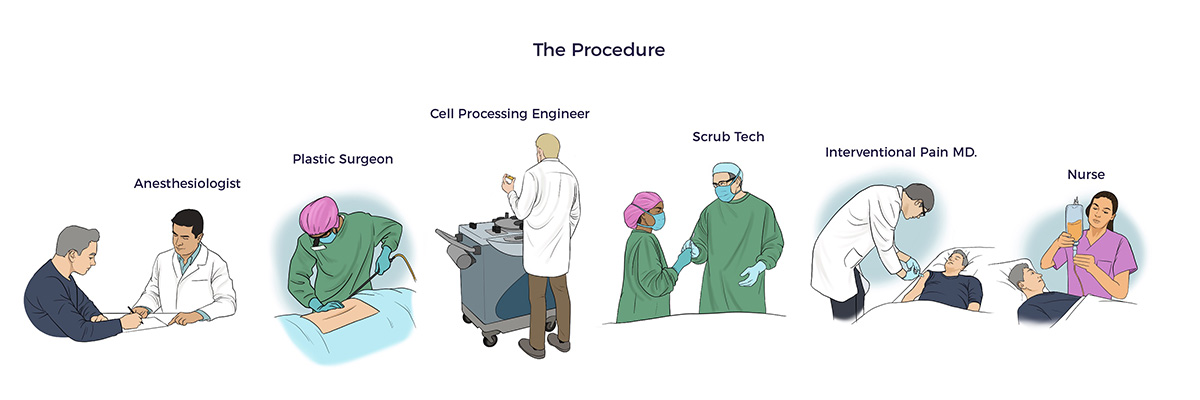
Un mes después de la operación, su fisioterapeuta dijo: "La tolerancia al peso y la condición física de Brian están mejorando. Lo está haciendo muy bien".
Después de ocho meses, Brian afirma: "Me siento bien en el hombro, las caderas y las rodillas. Mi espalda está bien".
Asma
Brian desarrolló asma a los 40 años tras pasar un mes en China por negocios. Antes del tratamiento con células madre, utilizaba tres inhaladores y tomaba 30 mg de prednisona al día.
Nueve meses después del tratamiento con AMBROSE, Brian afirma: "He reducido mi dosis diaria de prednisona a 10 mg y ocasionalmente dejo de tomarla sin que se produzca una crisis asmática. También he reducido significativamente el uso de inhaladores".
Fractura de costillas
Un ataque de tos inducido por el asma le fracturó cuatro costillas el 1 de marzo de 2018. Después de revisar las radiografías de Brian, su ortopedista le dijo que no podía reparar las costillas. Además, Brian tenía un diagnóstico subyacente de osteopenia, una afección que implica una reducción de la masa ósea.
Los estudios han demostrado que los ADRC estimulan la cicatrización ósea. [21]
El médico de Ambrose inyectó las costillas fracturadas. Varios meses después, Brian informó: "Siento que mis costillas se han curado. Es impresionante" Para ser claros, todavía experimenta ligeras molestias, "pero nada como antes".
Corazón ligeramente agrandado
Un estudio cardiológico realizado en 2018 reveló que Brian tenía un leve agrandamiento del corazón y dificultad para respirar.
Su cardiólogo y su fisioterapeuta coinciden en que la dificultad respiratoria ya no es evidente.
El estudio PRECISE de terapia celular cardiaca demostró mejoras significativas en la resistencia, lo que corrobora las observaciones del médico de Brian. [22] Un nuevo examen cardiaco es necesario.
Se restablece el equilibrio multisistema
Los resultados de los pacientes de Brian demuestran la posibilidad de restablecer la homeostasis multisistémica (equilibrio) utilizando sus ADRC.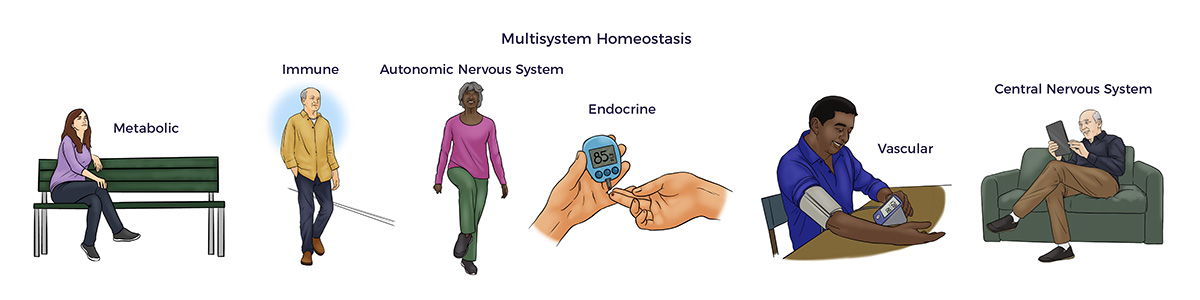
 Recomendar AMBROSE a familiares y amigos
Recomendar AMBROSE a familiares y amigos
"He recomendado Ambrose a mi madre y a mi mejor amiga. Tiene sentido que ellas también lo prueben. Ambas tienen articulaciones artríticas, dolor de espalda y otros problemas médicos."
[1] Yasamineh et al. Spotlight on therapeutic efficiency of mesenchymal stem cells in viral infections with a focus on COVID-19 Stem Cell Research & Therapy (2022) 13:257
[2] Wick K et al. Las células estromales mesenquimales reducen la evidencia de lesión pulmonar en pacientes con SDRA JCI Insight 2021;6(11):e148983
[3] Ross Eckard A, Borow KM, Mack EH, Burke E, Atz AM. Remestemcel-L therapy for
Síndrome inflamatorio multisistémico infantil asociado a COVID-19. Pediatrics. 2021
[4] Yilmaz R et al. Mesenchymal stem cells treatment in COVID-19 patient with multi-organ involvement Bratisl Med J 2020; 121 (12) 847-852
[5] Zeng et al. Transplantation of ACE2- Mesenchymal Stem Cells Improves the Outcome of Patients with COVID-19 Pneumonia Aging & Disease Volume 11 Number 2; 216-228, April 2020
[6] Fracción vascular estromal o SVF es el término genérico para las células regenerativas de grado clínico derivadas del tejido adiposo.
[7] Pietro Gentile, Aris Sterodimas. Adipose Stem Cells (ASCs) and Stromal Vascular Fraction (SVF) as a Potential Therapy in Combating (COVID-19)-Disease. Envejecimiento y enfermedad. 2020, 11(3): 465-469
[8] Alexander RW. (2020) Descripción general del ensayo clínico COVID-19 sobre daño pulmonar mediante células
Fracción vascular estromal (cSVF) y análisis de imágenes respiratorias funcionales (FRI) de la lesión pulmonar
Síndrome de distrés respiratorio del adulto (SDRA) postviral (SARS-CoV-2). Stem Cell Res. 1(1)-1-19.
[9] Sanchez-Guijo F et al. Células estromales mesenquimales derivadas de tejido adiposo para el tratamiento de pacientes con neumonía grave por SARS-CoV-2 que requieren ventilación mecánica. Un estudio de prueba de concepto EClinical Medicine 000 (2020) 100454
[10] S. Seigo et al, Uncultured adipose-derived regenerative cells promote peripheral nerve regeneration, Journal of Orthopaedic Science, Volume 18, Issue 1,2013, Pages 145-151.
[11] Xu et al El factor neurotrófico derivado del cerebro reduce la inflamación y la apoptosis del hipocampo en la meningitis experimental por Streptococcus pneumoniae Journal of Neuroinflammation (2017) 14:156
[12] Liao L. Mesenchymal stem cell and hematopoietic stem cell transplantation for vasculitis. Vasc Invest Ther 2020; 3:88-93.
[13] Jahangir S et al. New advanced therapy medicinal products in treatment of autoimmune diseases Editor(es): Nima Rezaei, In Translational Immunology, Translational Autoimmunity, Academic Press, Volume 2, 2022, Pages 319 359,
[14] Skok M. Mesenchymal stem cells as a potential therapeutic tool to cure cognitive impairment caused by neuroinflammation. World J Stem Cells 2021; 13(8): 1072-1083
[15] J Rosenstein, J Krum & C Ruhrberg VEGF en el sistema nervioso Organogenesis 6:2, 107-114; abril/mayo/junio 2010; © 2010 Landes Bioscience
[16] Nguyen A et al. Fracción vascular estromal: ¿Una realidad regenerativa? Parte 1: Conceptos actuales y revisión de la literatura Journal of Plastic, Reconstructive & Aesthetic Surgery (2016) 69, 170e179.
[17] Guo J et al. Fracción vascular estromal: ¿Una realidad regenerativa? Parte 2: Mecanismos de acción regenerativa Journal of Plastic, Reconstructive & Aesthetic Surgery (2016) 69, 180e188.
[18] Al-Ghadban S, Artiles M, Bunnell BA. Adipose Stem Cells in Regenerative Medicine: Looking Forward. Front Bioeng Biotechnol. 2022; 9:837464. Publicado el 13 de enero de 2022.
[19] Zhang, Y; Proenca, R; Maffei, M; Barone, M; Leopold, L; Friedman, JM (diciembre de 1994). "Positional cloning of the mouse obese gene and its human homologue". Nature. 1994 (372): 425-432
[20] Zuccarini, M et al Adipose Stromal/Stem Cell-Derived Extracellular Vesicles: Potenciales agentes antiobesidad de nueva generación. Int. J. Mol. Sci.
2022, 23, 1543.
[21] Saxer F et al. Implantation of Stromal Vascular Fraction Progenitors At Bone Fracture Sites: From A Rat Model To A First-In-Man Study STEM CELLS 2016; 00:00-00
[22] Perin E et al., Células regenerativas derivadas de tejido adiposo en pacientes con miocardiopatía isquémica: The PRECISE Trial Am Heart J 2014;168:88-95.e2.







 En el 86, el Parkinson había incapacitado, deprimido y herido a Mary. Los temblores le impedían usar tenedor y cuchillo.
En el 86, el Parkinson había incapacitado, deprimido y herido a Mary. Los temblores le impedían usar tenedor y cuchillo. En octubre de 2014, el grupo predecesor de Ambrose trató a Mary con un novedoso protocolo basado en el ADRC, que desencadenó su Regreso al Futuro. Siete años después de ese único tratamiento, Mary celebró su 93 cumpleaños con amigos.
En octubre de 2014, el grupo predecesor de Ambrose trató a Mary con un novedoso protocolo basado en el ADRC, que desencadenó su Regreso al Futuro. Siete años después de ese único tratamiento, Mary celebró su 93 cumpleaños con amigos. A medida que envejecemos, la situación se agrava: El anciano medio ve a siete médicos y toma siete medicamentos al año.
A medida que envejecemos, la situación se agrava: El anciano medio ve a siete médicos y toma siete medicamentos al año.
 A mediados de los años sesenta,
A mediados de los años sesenta, 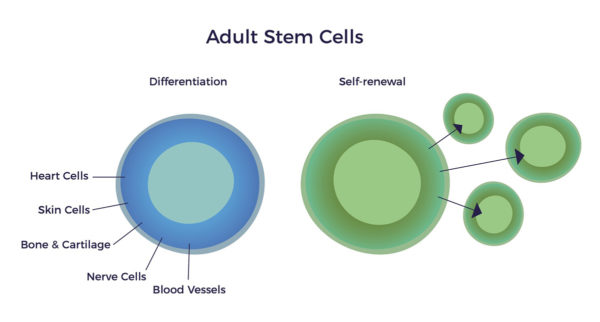
 Diez años después, los investigadores de la UCLA Patricia Zuk et al. descubrieron la fuente más accesible, abundante y potente de CMM: el tejido adiposo. El grupo de Zuk tendió un puente entre la ciencia milenaria de la fisiología y la medicina de la nueva era de las ADRC.
Diez años después, los investigadores de la UCLA Patricia Zuk et al. descubrieron la fuente más accesible, abundante y potente de CMM: el tejido adiposo. El grupo de Zuk tendió un puente entre la ciencia milenaria de la fisiología y la medicina de la nueva era de las ADRC. Las ADRC contienen ADN en el núcleo de cada célula. Por lo tanto, se adhieren al marco de la célula de señalización medicinal de Caplan.
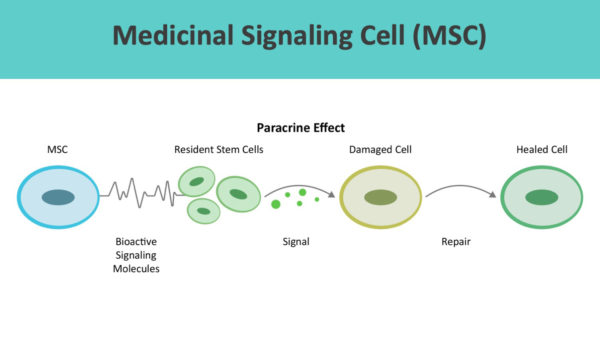
Las ADRC contienen ADN en el núcleo de cada célula. Por lo tanto, se adhieren al marco de la célula de señalización medicinal de Caplan.
 En 2006, el Dr. William Langston, primer Director Científico de la Fundación Michael J. Fox, publicó El Complejo de Parkinson: El Parkinsonismo es Sólo la Punta del Iceberg.
En 2006, el Dr. William Langston, primer Director Científico de la Fundación Michael J. Fox, publicó El Complejo de Parkinson: El Parkinsonismo es Sólo la Punta del Iceberg.  En pocas palabras, a medida que envejecemos, nuestras células, tejidos, órganos y sistemas pierden armonía.
En pocas palabras, a medida que envejecemos, nuestras células, tejidos, órganos y sistemas pierden armonía.  En términos científicos, sus células restauradoras segregaban cientos de factores curativos o tróficos que indicaban a las células residentes que volvieran a tocar según su partitura musical.
En términos científicos, sus células restauradoras segregaban cientos de factores curativos o tróficos que indicaban a las células residentes que volvieran a tocar según su partitura musical. En el mundo real, el estado de ánimo, la energía, el control motor, el equilibrio y la puntuación del dolor de Mary siguen mejorando desde hace más de siete años.
En el mundo real, el estado de ánimo, la energía, el control motor, el equilibrio y la puntuación del dolor de Mary siguen mejorando desde hace más de siete años.

 ¿Qué provoca un brote?
¿Qué provoca un brote?
 Aparentemente, Tony no sabía
Aparentemente, Tony no sabía 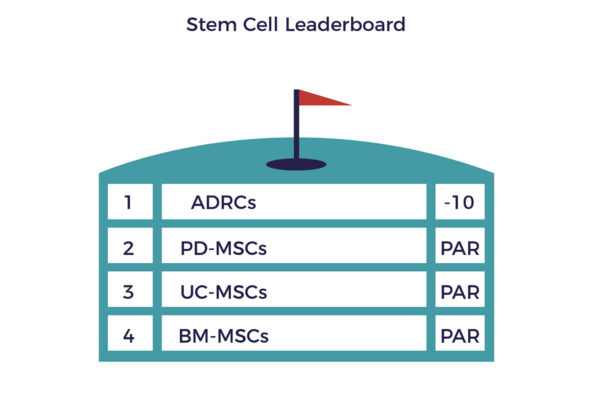 Nota, Jack dijo "me ayudó" - las células madre son el fertilizante - la terapia física, el ejercicio adecuado, y un estilo de vida saludable son los jardineros que restauran la salud.
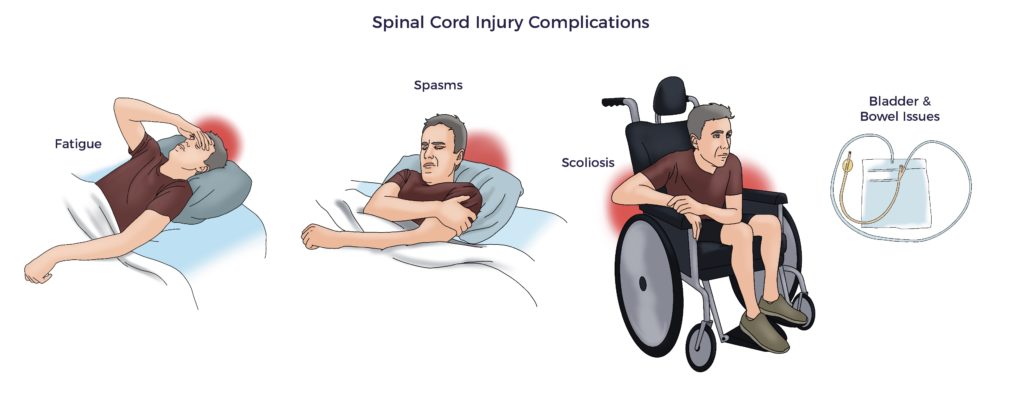
Nota, Jack dijo "me ayudó" - las células madre son el fertilizante - la terapia física, el ejercicio adecuado, y un estilo de vida saludable son los jardineros que restauran la salud.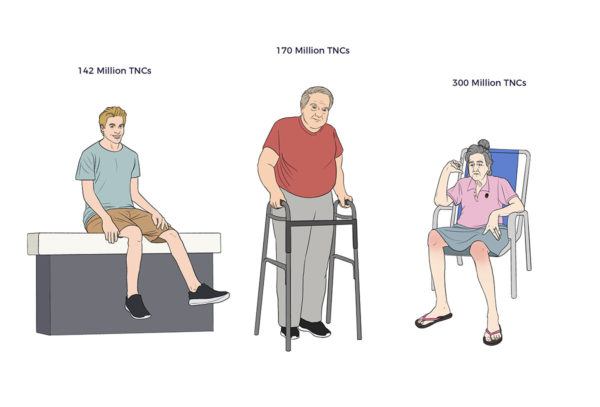 En la otra cara de la moneda, el rendimiento de un paciente de 15 años con lesión medular estaba a la altura de Bob. Seis meses después de la terapia celular y más de un año después de su catastrófica lesión, el joven recuperó el control motor bilateral de los flexores de la cadera y los cuádriceps. Los pacientes con lesiones medulares que reciben los cuidados estándar se estancan en torno a los 12 meses; sorprendentemente, la trayectoria de este joven se está acelerando.
En la otra cara de la moneda, el rendimiento de un paciente de 15 años con lesión medular estaba a la altura de Bob. Seis meses después de la terapia celular y más de un año después de su catastrófica lesión, el joven recuperó el control motor bilateral de los flexores de la cadera y los cuádriceps. Los pacientes con lesiones medulares que reciben los cuidados estándar se estancan en torno a los 12 meses; sorprendentemente, la trayectoria de este joven se está acelerando.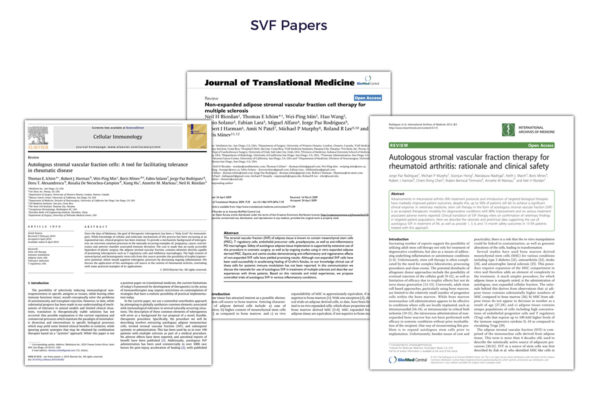 Investigaciones recientes aclaran que las células madre de donantes son "inmunoevasivas, no inmunoprivilegiadas", en contra de los defensores de la terapia celular alogénica.
Investigaciones recientes aclaran que las células madre de donantes son "inmunoevasivas, no inmunoprivilegiadas", en contra de los defensores de la terapia celular alogénica.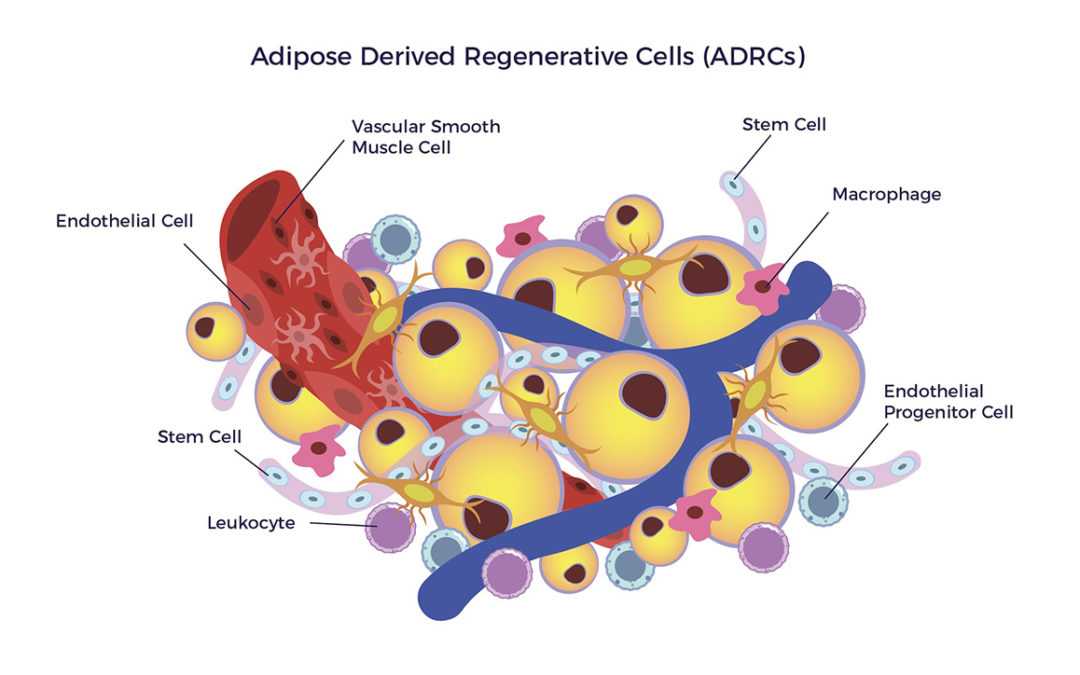
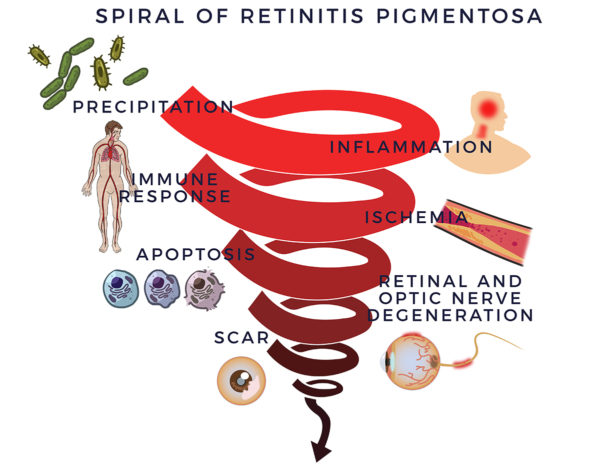 En 1857, el Dr. Donders identificó un grupo de trastornos oculares incurables a los que denominó retinosis pigmentaria (RP). Pero no era tan sencillo: Posteriormente, los investigadores descubrieron más de 100 genes que pueden contener mutaciones que provoquen retinosis pigmentaria. Pero las anomalías genéticas no lo aclaran todo; la mitad de los casos de RP carecen de antecedentes familiares y explicaciones previas.
En 1857, el Dr. Donders identificó un grupo de trastornos oculares incurables a los que denominó retinosis pigmentaria (RP). Pero no era tan sencillo: Posteriormente, los investigadores descubrieron más de 100 genes que pueden contener mutaciones que provoquen retinosis pigmentaria. Pero las anomalías genéticas no lo aclaran todo; la mitad de los casos de RP carecen de antecedentes familiares y explicaciones previas.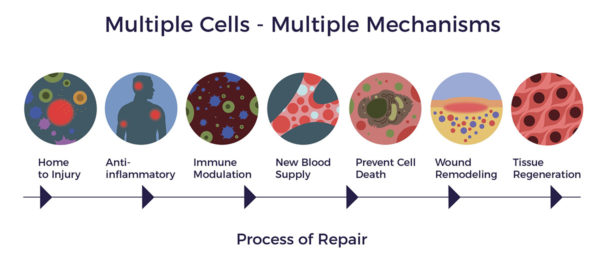
 Los desarrolladores de fármacos y terapias génicas siguen persiguiendo el fallido modelo de "una molécula o un gen para una enfermedad" para la RP. Este enfoque minimalista no ha producido ningún fármaco o terapia génica que modifique la progresión de la enfermedad o mejore la agudeza visual mejor corregida (AVMC) de los pacientes.
Los desarrolladores de fármacos y terapias génicas siguen persiguiendo el fallido modelo de "una molécula o un gen para una enfermedad" para la RP. Este enfoque minimalista no ha producido ningún fármaco o terapia génica que modifique la progresión de la enfermedad o mejore la agudeza visual mejor corregida (AVMC) de los pacientes.
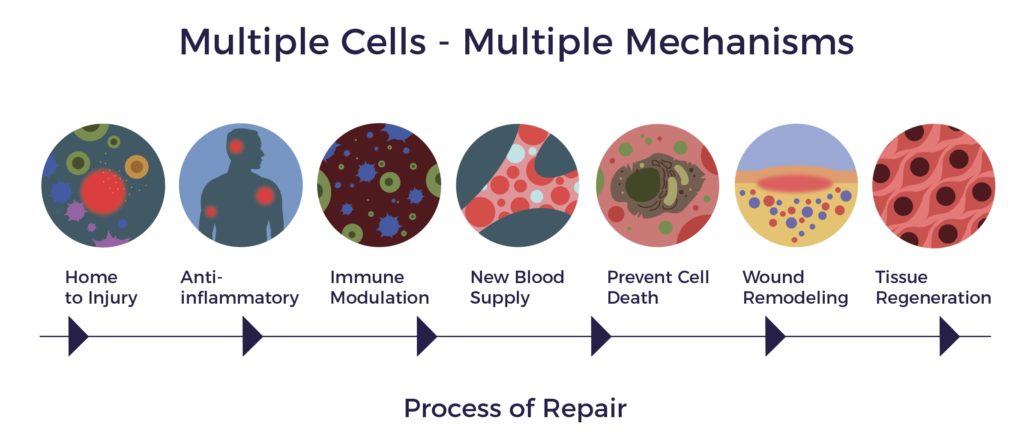
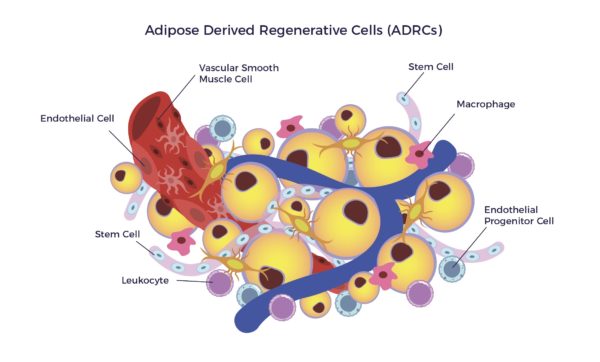
 Las ADRC son una población heterogénea de células, que incluye células madre mesenquimales, otras células progenitoras, fibroblastos, células reguladoras T y macrófagos. La mezcla incluye un alto porcentaje de células endoteliales, células progenitoras endoteliales, macrófagos y leucocitos.
Las ADRC son una población heterogénea de células, que incluye células madre mesenquimales, otras células progenitoras, fibroblastos, células reguladoras T y macrófagos. La mezcla incluye un alto porcentaje de células endoteliales, células progenitoras endoteliales, macrófagos y leucocitos.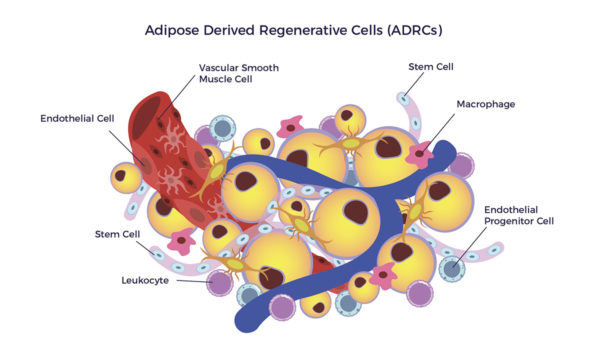 Tras recibir una señal inflamatoria, el secretoma de las ADRC libera cientos de citocinas y factores de crecimiento en el microentorno enfermo. Las células endógenas envían señales a los ADRC.
Tras recibir una señal inflamatoria, el secretoma de las ADRC libera cientos de citocinas y factores de crecimiento en el microentorno enfermo. Las células endógenas envían señales a los ADRC.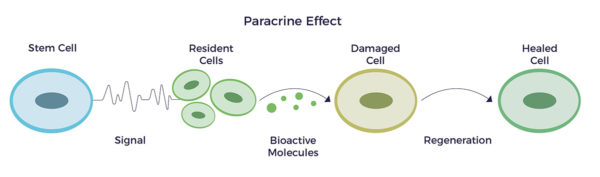
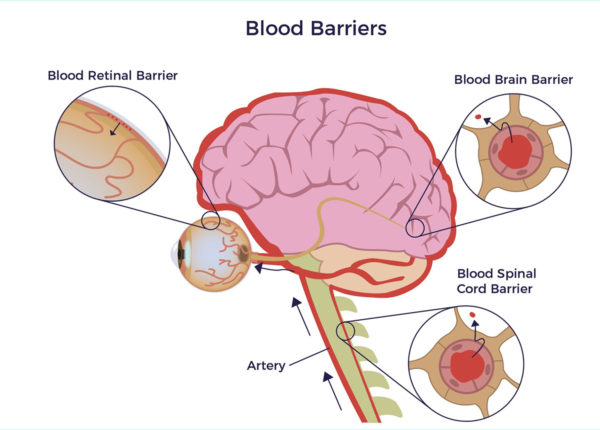 Permeabilidad de la barrera hemato-retiniana
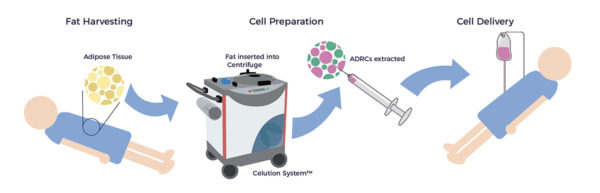
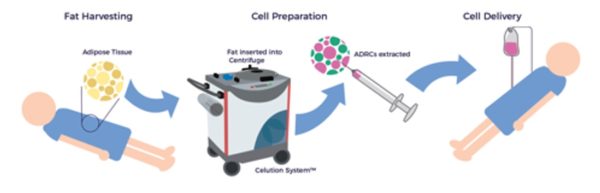
Permeabilidad de la barrera hemato-retiniana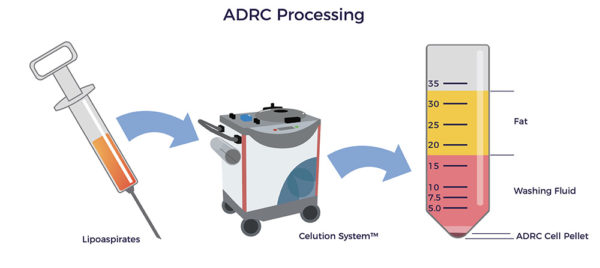 Más de 40 países han aprobado el uso clínico de Celution, entre ellos el Reino Unido, la Unión Europea, Japón, Corea del Sur y Nueva Zelanda. Además, la FDA ha aprobado Celution para nueve ensayos clínicos.
Más de 40 países han aprobado el uso clínico de Celution, entre ellos el Reino Unido, la Unión Europea, Japón, Corea del Sur y Nueva Zelanda. Además, la FDA ha aprobado Celution para nueve ensayos clínicos.
 Pero el anciano medio ve a siete médicos y toma siete medicamentos al año. Así pues, todos conocemos a alguien -o somos ese alguien- que vive con una mala calidad de vida.
Pero el anciano medio ve a siete médicos y toma siete medicamentos al año. Así pues, todos conocemos a alguien -o somos ese alguien- que vive con una mala calidad de vida. Los biocientíficos autoproclamados están en el otro extremo del espectro.
Los biocientíficos autoproclamados están en el otro extremo del espectro. Si algo puede ayudar a tu salud -sin necesidad de pruebas- uno de los biocientíficos lo venderá o promocionará. Al hacerlo, afirman que sus productos, equipos, libros, podcasts y drogas psicodélicas son la solución para todo, desde las enfermedades crónicas hasta el envejecimiento saludable.
Si algo puede ayudar a tu salud -sin necesidad de pruebas- uno de los biocientíficos lo venderá o promocionará. Al hacerlo, afirman que sus productos, equipos, libros, podcasts y drogas psicodélicas son la solución para todo, desde las enfermedades crónicas hasta el envejecimiento saludable.
 Al igual que las grandes farmacéuticas, el biohacking es un gran negocio. Si apiláramos unos encima de otros todos los equipos, productos, suplementos, café, alimentos, libros, materiales de cursos, documentos de franquicia, entradas de blog y transcripciones que comercializan las tres grandes, tendría la altura de una supertienda de 10 plantas.
Al igual que las grandes farmacéuticas, el biohacking es un gran negocio. Si apiláramos unos encima de otros todos los equipos, productos, suplementos, café, alimentos, libros, materiales de cursos, documentos de franquicia, entradas de blog y transcripciones que comercializan las tres grandes, tendría la altura de una supertienda de 10 plantas. Los polos opuestos son las estrellas de la fórmula "volver a lo básico". Son personas corrientes que disfrutan de la vida hasta los 80, 90 y 100 años con recuerdos intactos, corazones sanos y una vida social enriquecedora.
Los polos opuestos son las estrellas de la fórmula "volver a lo básico". Son personas corrientes que disfrutan de la vida hasta los 80, 90 y 100 años con recuerdos intactos, corazones sanos y una vida social enriquecedora. A título personal, los pilares del Poder de la Simplicidad abarcan el futuro de un envejecimiento saludable, feliz y digno. Y puedes derrochar en ellos sin tener que gastar dinero en la Biohacking Superstore.
A título personal, los pilares del Poder de la Simplicidad abarcan el futuro de un envejecimiento saludable, feliz y digno. Y puedes derrochar en ellos sin tener que gastar dinero en la Biohacking Superstore.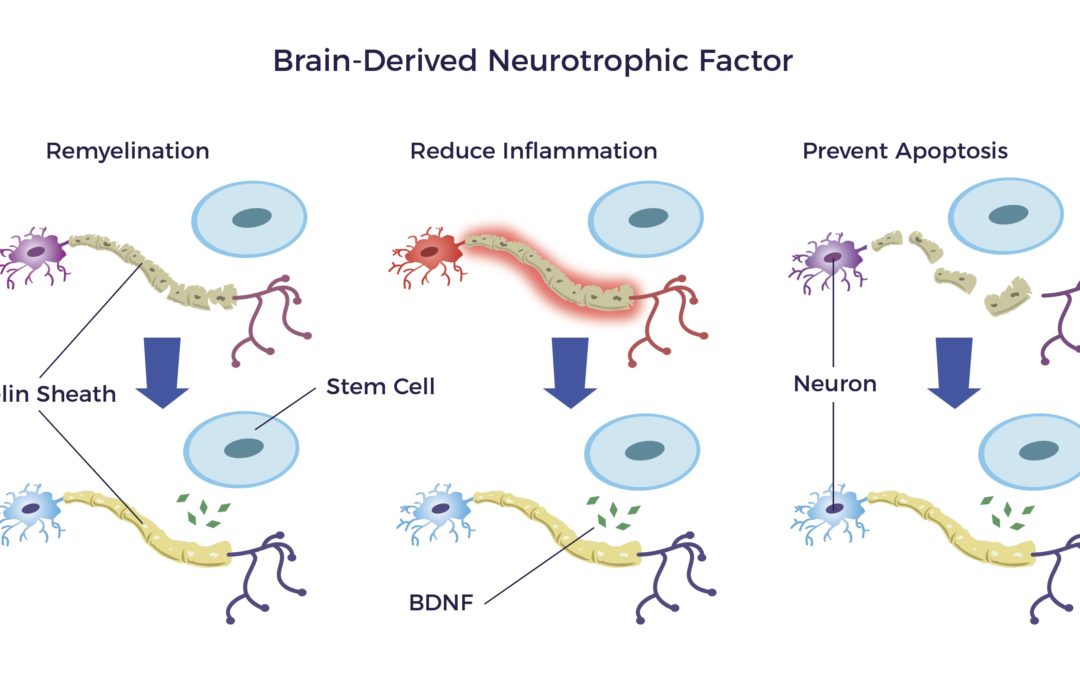



 La hazaña de Alexander es trivial comparada con desatar la intrincada red de enredos que supone atender a pacientes sin opción. Este dilema es aún más complicado de lo que puede parecer a primera vista.
La hazaña de Alexander es trivial comparada con desatar la intrincada red de enredos que supone atender a pacientes sin opción. Este dilema es aún más complicado de lo que puede parecer a primera vista.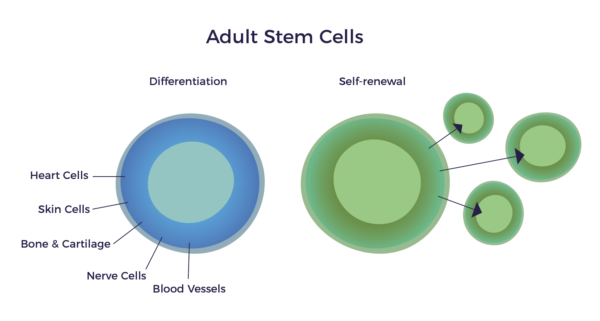
 Como testimonio de la visión y la investigación del Dr. Caplan, según un
Como testimonio de la visión y la investigación del Dr. Caplan, según un 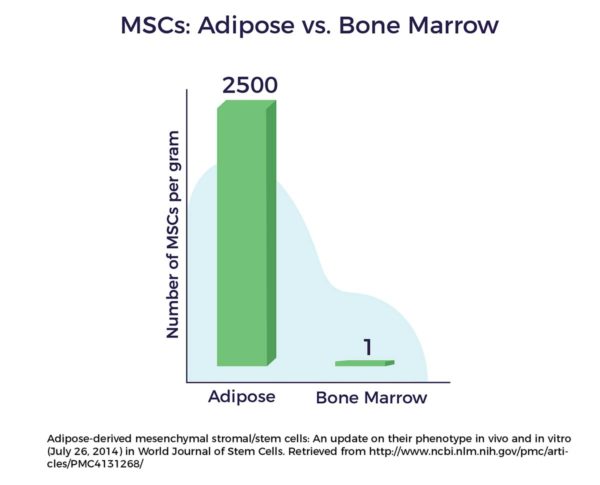
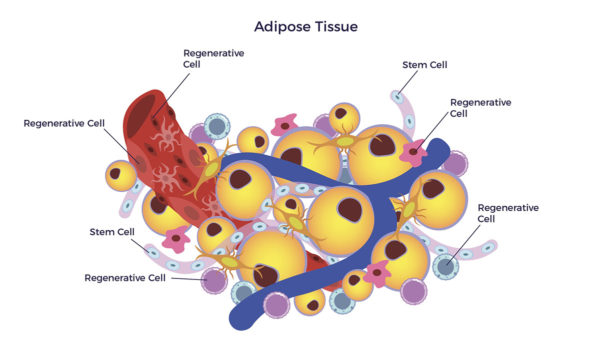
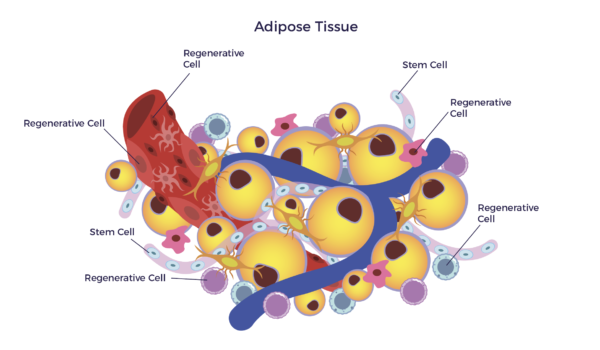 En otras palabras, existe una población mixta de células madre y otras células regenerativas en nuestra grasa. En el ámbito clínico, esta mezcla diversa de células se denomina Adipose-Derivado Regenerativo Cells (ADRC).
En otras palabras, existe una población mixta de células madre y otras células regenerativas en nuestra grasa. En el ámbito clínico, esta mezcla diversa de células se denomina Adipose-Derivado Regenerativo Cells (ADRC).