فرضية العلاج الخلوي لإصابات الحبل الشوكي
فرضية العلاج الخلوي لإصابات الحبل الشوكي
الخلفية: في ديسمبر 2018، كان العلاج بالخلايا من AMBROSE رائداً في بروتوكول جديد لجيف، وهو مريض يعاني من إصابة في الحبل الشوكي. النتائج التي أبلغ عنها جيف لمدة 14 شهراً من تقرير المريض سجلت تحسنًا ملحوظًا في الأعراض والوظائف وجودة الحياة.
في ديسمبر 2017، نتج عن جراحة العمود الفقري التي أُجريت لجيف في ديسمبر 2017 خطأ جراحي في العمود الفقري أدى إلى إصابته بشلل نصفي. وأدى دخوله المستشفى لفترة طويلة إلى إصابته بخرّاج في القولون مما استدعى إجراء فغر اللفائفي. ومما زاد الأمر تعقيداً أنه كان يعاني من داء السكري من النوع الثاني.
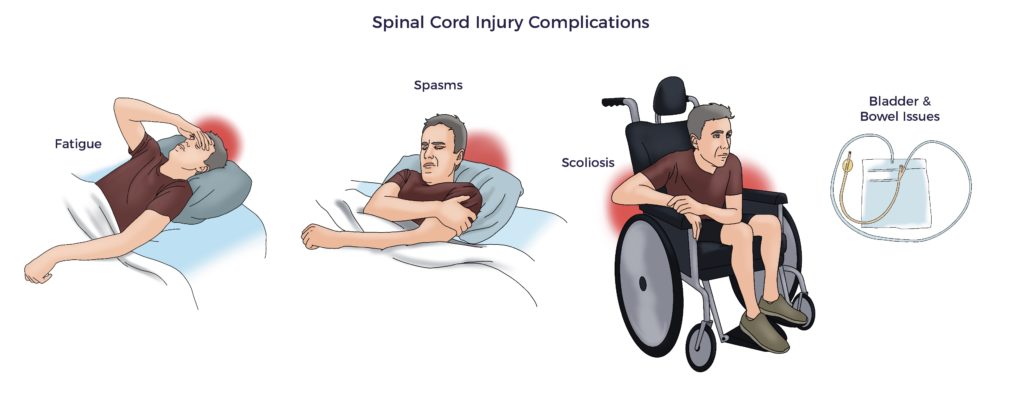
اشتكى جيف من آلام الرقبة والظهر والاعتلال العصبي وألم الندبة الناتجة عن فغر اللفائفي وأصابع القدمين التشنجية وضعف التوازن ومرض السكري T2 وعدم حركة الكتف وضعف الانتصاب (ED). تناول سبعة أدوية للسيطرة على أعراضه، بما في ذلك المسكنات الأفيونية.
وقد أسفرت مراجعتنا المتعمقة لدراسات العلاج بالخلايا الجذعية المنشورة عن نتائج إيجابية. وهكذا، قام مركز AMBROSE بتنسيق الأدبيات وتطوير علاج مخصص البروتوكول لـ جيف
كانت استراتيجية العلاج غير تقليدية. فبدلاً من استهداف آفة النخاع الشوكي فقط، عالج فريق AMBROSE الطبي مجموعة من شكاوى جيف في إجراء واحد باستخدام البروتوكول الرئيسي.
في الأساس، صممت AMBROSE بروتوكولاً شاملاً واحداً لعلاج مشاكل متعددة في علاج واحد بما في ذلك موقع الإصابة، باستخدام الخلايا المتجددة المشتقة من الدهون (ADRCs). ثم يقوم فريق العلاج لدينا بتخصيصه لكل مريض.
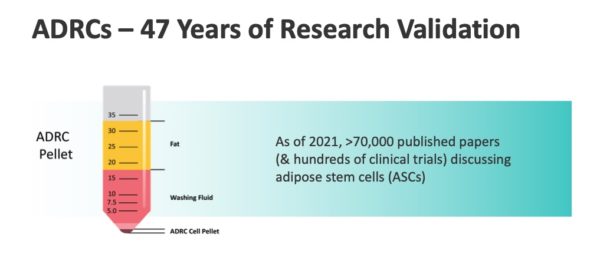
والأهم من ذلك، أن النجاحات السابقة التي حققتها مجموعتنا السابقة باستخدام بروتوكول رئيسي مع أكثر من 300 مريض يعانون من حالات مزمنة متنوعة دعمت فرضيتنا. (Okyanos Cell Therapy، جزر البهاما 2014-2017).
بالإضافة إلى ذلك:
- تحليل تلوي لاحق, زرع الخلايا الجذعية الوسيطة الوسيطة لإصابات الحبل الشوكي: مراجعة منهجية وتحليل تلوي شبكي, التحقق من صحة سلامة وفعالية العلاجات القائمة على الخلايا الجذعية الصلبة في علاج التهاب الحبل الشوكي. [1]
- نشر باحثون تقارير حالات ناجحة باستخدام حقن الأنسجة الدهنية المجهرية لمعالجة الحالات المرضية العضلية الهيكلية المرتبطة بالإصابة بالشلل الرقعي وآلام الندبات والاعتلال العصبي. [2] [3]
- التجارب المنشورة للحالات المزمنة الأخرى التي تم إبلاغك بها.[4] [5]
- نصح أخصائيو المسالك البولية ببروتوكول فرعي لحقن الضفيرة العجزية لاستهداف الخلل الوظيفي في المثانة والأمعاء.
الفرضية
توجد فجوة واسعة بين الفيزيولوجيا المرضية المعروفة لإصابة الحبل الشوكي ومعيار الرعاية الذي يتم الاعتماد عليه في علاجها. وعلى وجه التحديد، يؤدي تلف الحبل الشوكي إلى حدوث خلل في أجهزة الجسم المتعددة، بما في ذلك الخلل الوظيفي المناعي والبطاني والاستقلابي والميتوكوندريا والخلل الوظيفي اللاإرادي. [6] [7] [8]
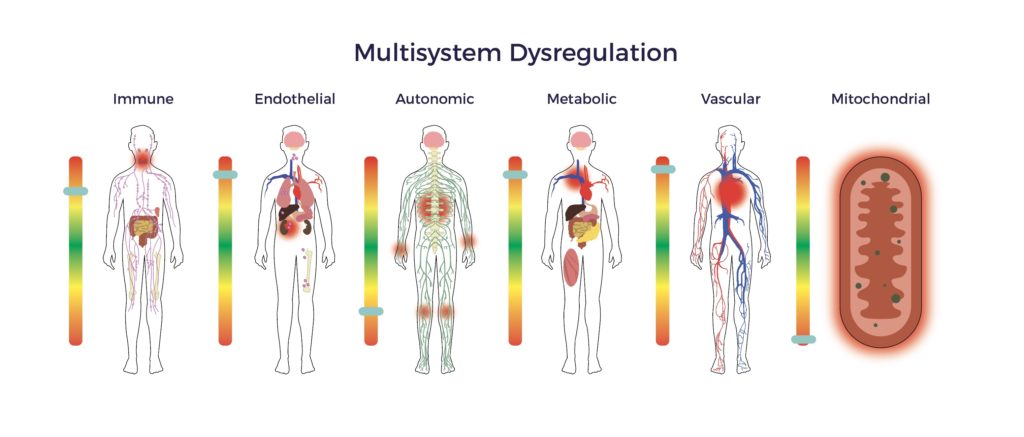
وبالتالي، يعاني المرضى من مجموعة من المضاعفات الثانوية.
وعلاوة على ذلك، فإن الإهانة الساحقة تكبح تجدد الحبل الشوكي، مما يحد من التعافي الوظيفي. وبالتالي، فإن فترة التحسن المتوقعة لمرضى إصابات النخاع الشوكي الشوكي هي 12 شهراً تقريباً.
على سبيل المثال، شملت أعراض جيف ألم الندبة على مدار الساعة طوال أيام الأسبوع، والاعتلال العصبي، والتشنج الثنائي، ومشاكل الأمعاء والمثانة، والضعف الجنسي وضعف التوازن. بعد مرور 11 شهرًا على الإصابة، أدرك جيف وطبيبه الفيزيائي أن تقدمه قد استقر.
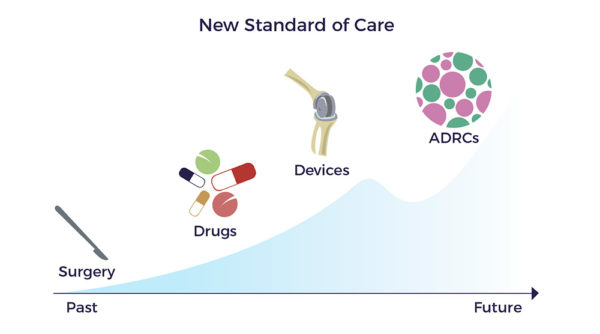
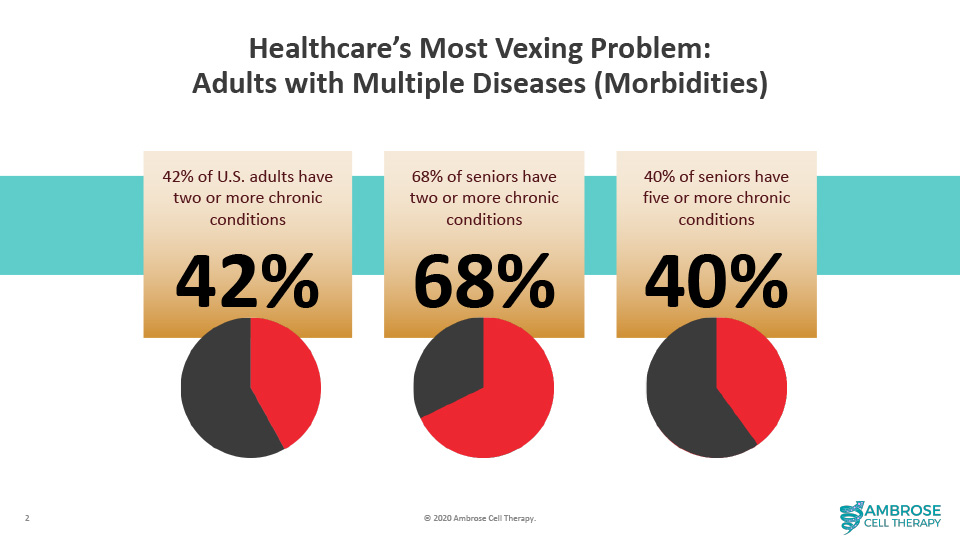
ومع ذلك، فإن اكتشاف الأدوية يركز على آلية عمل واحدة لإصلاح موقع الإصابة أو قمع أحد الأعراض. وبعبارة أخرى، لم يحرز النموذج الدوائي الذي يعتمد على دواء أو جين أو نوع واحد من الخلايا لعلاج المرض سوى تقدم ضئيل في تحسين تشخيص المرضى الذين يعانون من إصابات الحبل الشوكي. يتجاهل هذا النهج مجموعة كبيرة من الأدبيات التي توثق العوامل المتعددة والأمراض المصاحبة الناتجة التي تجتمع لتُعيق المرضى مثل جيف.
الآليات المتعددة لمراكز إعادة التأهيل والتطوير
وعلى النقيض من ذلك، فإن أدوية علاج الأمراض المزمنة لها آليات عمل متعددة (MOAs) تستهدف جميع العوامل التي تنطوي عليها الحالة المزمنة، بما في ذلك خلل في تنظيم الأجهزة المتعددة. [9]
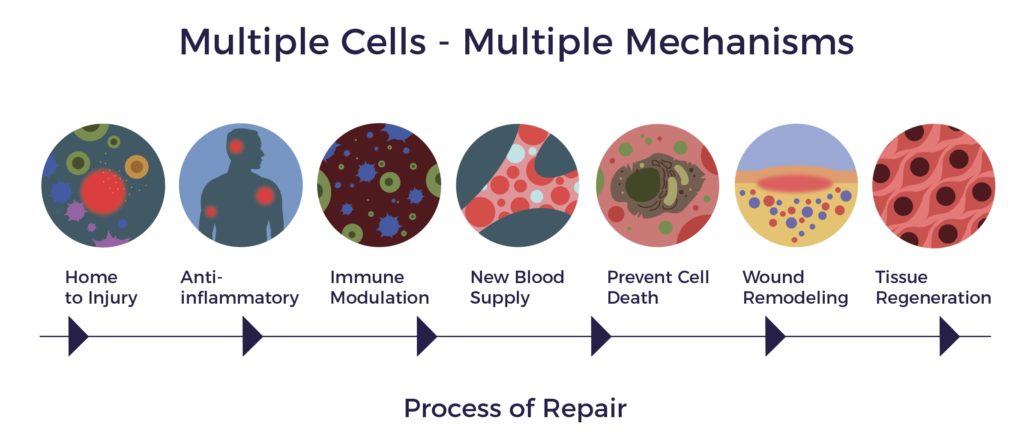
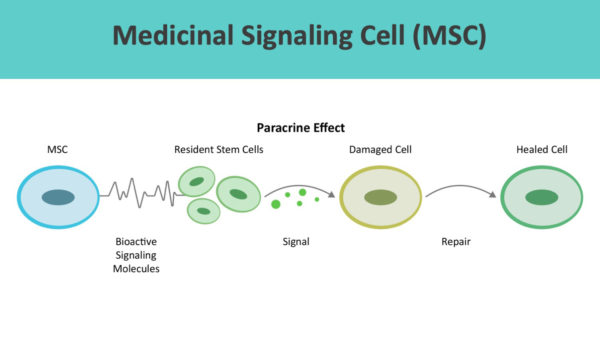
تستوطن مراكز علاج الالتهابات في مواقع الالتهاب وتفرز المئات من الجزيئات النشطة بيولوجيًا والمضادة للالتهابات والمعدلة للمناعة والمولدة للأوعية والمضادة للاستماتة والمضادة للاستماتة والتئام الجروح.
تعمل ADRCs من خلال التواصل من خلية إلى خلية أو التأثير الباراكريني.
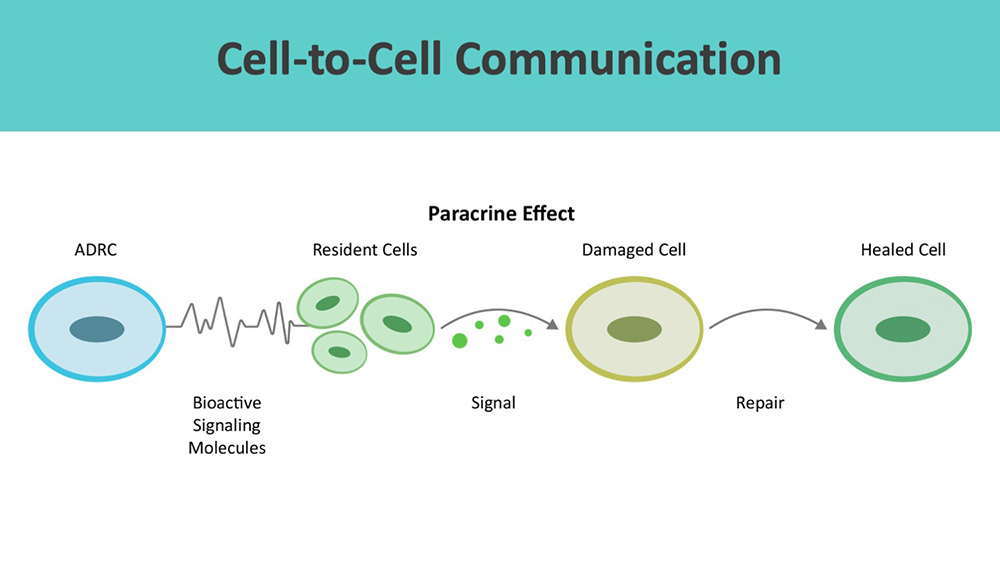
وبعيدًا عن آليات التئام الجروح، تستعيد مراكز علاج الإصابات والجروح التوازن الخلوي والجهازي والأنسجة (التوازن متعدد الأجهزة). [10] [11]
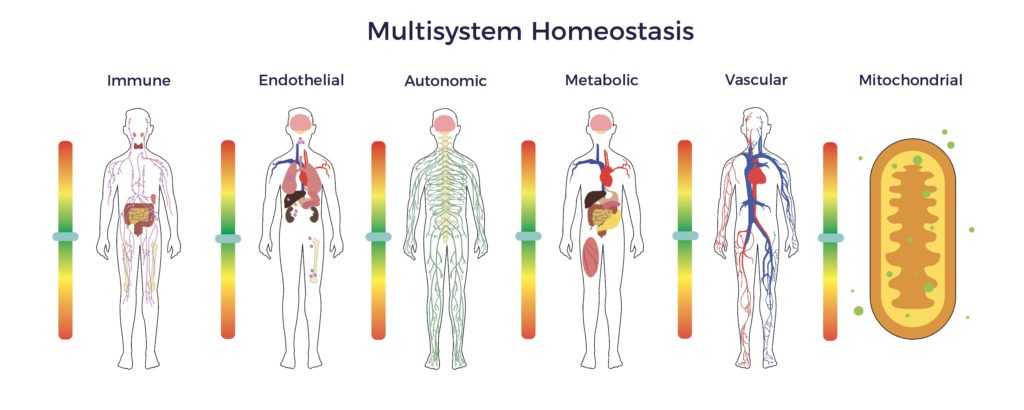
في فترة تعافي جيف، تضمنت استعادة التوازن متعدد الأجهزة تحسين التوازن ودرجات الألم ووظائف المثانة والأمعاء، بالإضافة إلى انخفاض كبير في التشنج. وكانت النتيجة الصافية هي الاستغناء عن جميع الأدوية، والانخراط في تمارين رياضية قوية، والعودة إلى السباقات، وتعلم قيادة المروحيات والغوص، بالإضافة إلى لعب الغولف ثلاث مرات في الأسبوع. على الرغم من عدم شفاء جيف أو عدم ظهور الأعراض، إلا أنه دليل واقعي على أن برنامج ADRCs مدد فترة تعافي جيف.
وباختصار، تشير الأدلة الأولية التي توصلنا إليها إلى أن مراكز علاج الإدمان يمكن أن تمدد أو تعيد تشغيل نافذة التعافي العصبي من خلال استعادة التوازن متعدد الأجهزة.
لماذا الأنسجة الدهنية؟
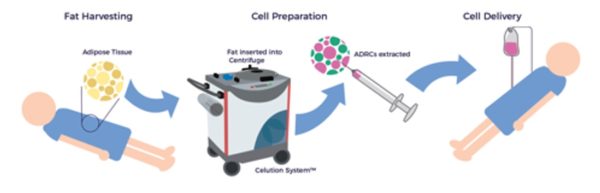
وخلافًا لمصادر الأنسجة الأخرى للخلايا الجذعية للبالغين، مثل نخاع العظم، تظل الخلايا الجذعية الوراثية النخاعية البديلة متاحة ومتوفرة وفعالة طوال حياة الشخص. [12] بعد شفط الدهون، يقوم نظام معالجة الخلايا Celution™ Cell Processing System (Lorem Cytori, Inc.) بالطرد المركزي للنضح الشحمي وتحضير الخلايا الشحمية الملقحة.
لماذا مراكز الاستجابة للطوارئ الطارئة
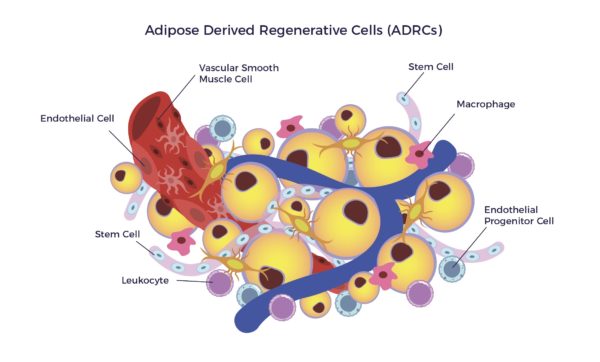
Aثنائي البوصة-Dمشتق Rالتوليد Cالخلايا الوعائية اللحمية الوعائية (ADRCs) هي تسمية لمستحضر سريري من الدرجة السريرية للجزء الوعائي اللحمي (SVF)، وهي مجموعة غير متجانسة من الخلايا الموجودة على البطانة الخارجية للشعيرات الدموية في الأنسجة الدهنية. يتضمن مزيج الخلايا الخلايا الخلايا الجذعية الصلبة متعددة الخلايا والخلايا البطانية (ECs) والخلايا السلفية البطانية (EPCs) والخلايا الليفية والخلايا التائية المنظمة (Tregs) والخلايا الضامة والخلايا المناعية الأخرى (الكريات البيض).[13]
تفرز الخلايا الجذعية الصلبة الأذينية المتصلبة المستمدة من الدهون كميات أكبر بكثير من العوامل الغذائية مقارنةً بالخلايا الجذعية الصلبة المشتقة من الدهون.[14] ولذلك، فإن إفرازات مركز أبو ظبي للبحوث والإنقاذ تضخّم من عمل الخلايا الجذعية في الخلايا الجذعية في الدماغ، بما في ذلك على سبيل المثال لا الحصر:
- مضادات الالتهاب والتعديل المناعي,
- مضاد للاستماتة,
- تولد الأوعية الدموية,
- دعم النمو,
- تمايز الخلايا الجذعية المحلية والخلايا السليفة,
- مضاد للندوب، و
- الجذب الكيميائي.
تظهر الدراسات التي أجريت على البشر
- إطلاق العوامل التي تقلل من تنظيم علامات الالتهاب المناعة الذاتية، بما في ذلك على سبيل المثال لا الحصر TNF-A وTH17 و IL6 و IL2، بالإضافة إلى زيادة تنظيم IL10.
- تعزيز التحول من البلاعم الالتهابية (M1s) إلى البلاعم المضادة للالتهابات (M2s) عن طريق البروستاغلاندين E2 (PGE2) والمواد البلعمية الصلبة متعددة الخلايا في المزيج.
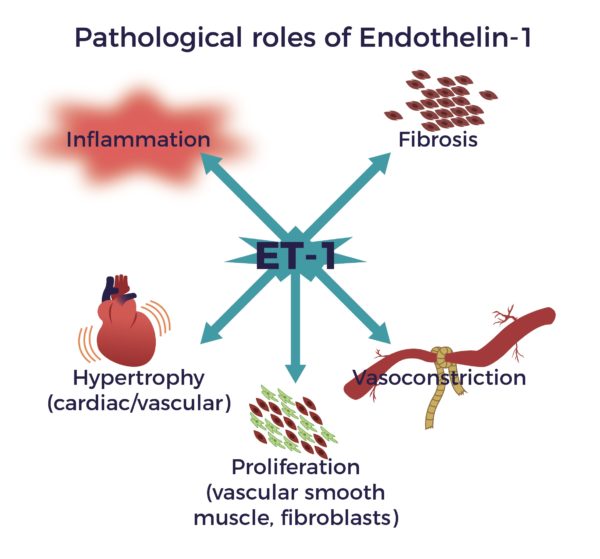
- تقليل هرمون الإندوثيلين-1 (ET-1)، وهو مقلص معروف للأوعية الدموية، وهو متورط في اضطراب الحاجز الدموي للحبل الشوكي بعد الإصابة.
- المساعدة في نمو الأوعية الدموية الجديدة وتثبيتها عن طريق إفراز عامل النمو المشيمي (PGF) والعامل المشتق من الأنسجة اللحمية-1 (SDF-1) وعامل النمو البطاني الوعائي (VEGF).
وتجدر الإشارة إلى وجود علاقة وثيقة بين إعادة الأوعية الدموية وتحسن النتائج الوظيفية بعد الإصابة بالشلل النخاعي. أولاً، توفر الآفة ذات الأوعية الدموية الجيدة بيئة مجهرية متساهلة لبقاء الأنسجة المحلية وتجديد الأعصاب. ويؤدي تحسين تدفق الدم الشعري وتكوين الأوعية الدموية وسلامة B-SC-B إلى تسهيل التعافي الوظيفي.[15] [16]
عوامل التغذية العصبية
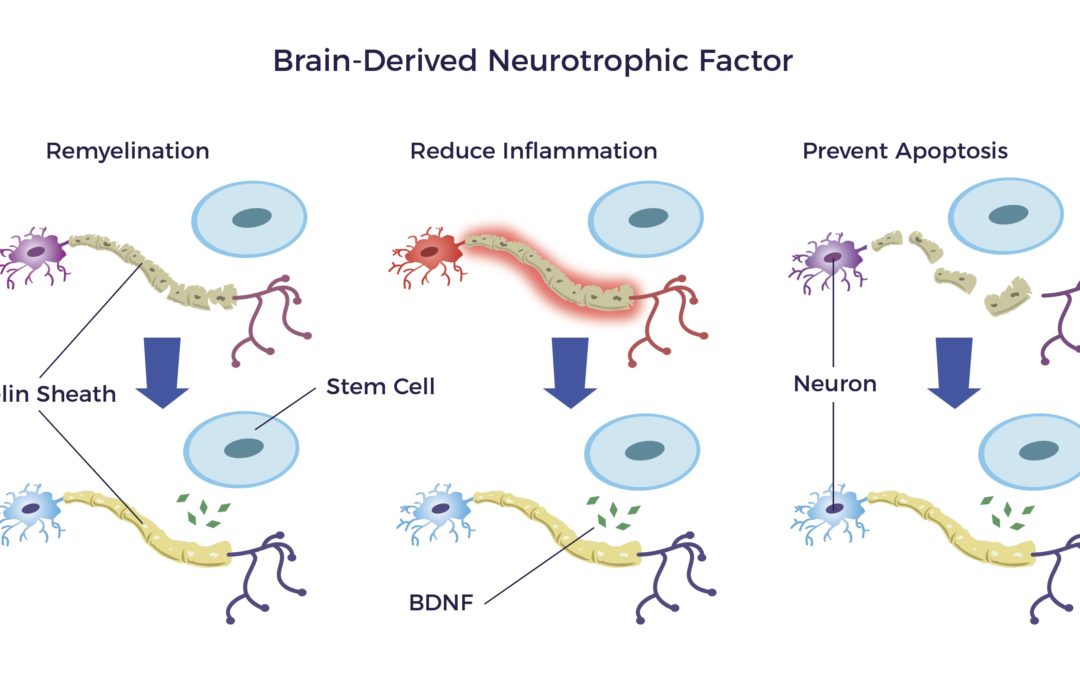
تقدم ADRCs عوامل التغذية العصبية (NTFs) إلى الجهاز العصبي المركزي والجهاز العصبي المركزي والجهاز العصبي العصبي المحيطي والجهاز العصبي العصبي المركزي. تماماً كما تحافظ الأسمدة على صحة النباتات ونموها، تحفز عوامل التغذية العصبية نمو خلايا دماغية جديدة وتوصيلات خلايا الدماغ والأعصاب.
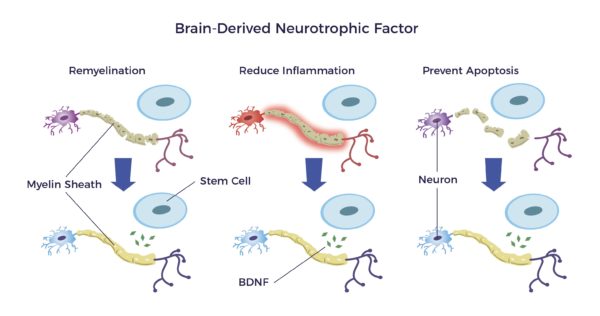
أحد هذه العوامل الغذائية هو عامل التغذية العصبية المشتق من الدماغ أو BDNF.
BDNF:
- إصلاح غلاف النخاعين المحيط بالأعصاب
- يقلل من الالتهاب و,
- يمنع موت الخلايا المبرمج الناتج عن إصابة أو مرض. [17] [18] [19] [20] [21]
ويربط الاكتشاف الأخير للخلايا العصبية المناعية العصبية في مركز أبحاث أمراض الجهاز العصبي المركزي بين دورها في تعزيز المرونة العصبية.[22] [23]
السلامة
منذ عام 2007، لم يتم الإبلاغ عن أي أحداث عكسية مرتبطة ب ADRC.[24]
[1] تشين وآخرون زراعة الخلايا الجذعية الوسيطة الوسيطة لإصابة الحبل الشوكي: مراجعة منهجية وتحليل تلوي شبكي J Transl Med (2021) 19:178
[2] شيريان سي وآخرون. الأنسجة الدهنية المجزأة الدقيقة الذاتية كعلاج لآلام الكتف المزمنة لدى شخص يستخدم الكرسي المتحرك مصاب بإصابة في الحبل الشوكي: تقرير حالة سلسلة وحالات الحبل الشوكي (2019) 5:46
[3] Huang S-H, Wu S-H, Lee S-S, Chang K-P, Chai C-Y, Yeh J-L, et al. (2015) تطعيم الدهون في ندبة الحرق يخفف من الألم العصبي عن طريق تأثير مضاد للالتهاب في الندبة والحبل الشوكي. PLoS ONE 10(9): e0137563
[4] A Nguyen, A et al جزء الأوعية الدموية اللحمية: واقع متجدد؟ الجزء 1: المفاهيم الحالية ومراجعة الأدبيات مجلة الجراحة التجميلية والترميمية والتجميلية (2016) 69, 170e179
[5] قوه وآخرون جزء الأوعية الدموية اللحمية: واقع متجدد؟ الجزء 2: المفاهيم الحالية ومراجعة الأدبيات مجلة الجراحة التجميلية والترميمية والتجميلية (2016) 69, 180e188
[6] سون وآخرون. الخلل الوظيفي للأعضاء المتعددة والالتهاب الجهازي بعد إصابة الحبل الشوكي: علاقة معقدة مجلة الالتهاب العصبي (2016) 13:260:13
[7] B. P. Perrouin-Verbe، C. Lefevre، P. Kieny، R. Gross، B. Reiss، M. Le Fort، إصابة الحبل الشوكي: ضعف/خلل وظيفي فسيولوجي متعدد الأنظمة، مجلة الأعصاب، المجلد 177، العدد 5، 2021، الصفحات 594 605,
[8] ماريون وآخرون. الأحداث الضائرة الشائعة التي تم تحديدها سابقًا بعد الإصابة في إصابات الحبل الشوكي الرضحية - التحقق من صحة الأدبيات الموجودة وعلاقتها بأمراض مصاحبة مختارة قابلة للتعديل: دراسة جماعية كندية مستقبلية دراسة جماعية كندية JOURNAL OF NEUROTRAUMA 34:2883-2891 (15 أكتوبر 2017)
[9] كابلان أ I الخلايا الجذعية الوسيطة: حان الوقت لتغيير الاسم! الخلايا الجذعية translationalmedicine 2017; 6:1445-1451
[10] فيسوسو ف. ج. وآخرون الخلايا الجذعية الوسيطة في التوازن والأمراض الجهازية: الفرضيات والأدلة والفرص العلاجية Int. J. Mol. Sci. 2019, 20, 3738
[11] Morris, M.E. et al. (2015)، خلايا الأوعية الدموية اللحمية الدهنية الوعائية التي يتم توصيلها بشكل منهجي تنتشر في جدران الشرايين المحيطية وتقلل من التوتر الحركي الوعائي من خلال CD11b+ الآلية المعتمدة على الخلية. STEM CELLS CELLS Translational Medicine, 4: 369-380.
[12] Perin EC و Willerson JT Buying New Soul J Am Coll Cardiol. 2012;60(21):2250-2251
[13]إس كيستن وجيه كيه فريزر الخلايا التجددية الذاتية المشتقة من الدهون: منصة للتطبيقات العلاجية التكنولوجيا الجراحية الدولية المتقدمة لالتئام الجروح الجراحية XXIX
[14] Hirosi Y وآخرون. مقارنة بين العوامل الغذائية المفرزة من الجزء الوعائي المشتق من الخلايا الجذعية/الجذعية المشتقة من الخلايا الجذعية/الجذعية الدهنية البشرية في نفس الأفراد
[15]Yao C، و Cao X و Yu B (2021) إعادة التوعّي بعد إصابة الحبل الشوكي الرضحية. Front. Physiol. 12:631500.
[16] نعمان إم تي وآخرون. العلاج بالخلايا الجذعية الدهنية الذاتية لخلل وظيفي في الجهاز العصبي اللاإرادي لدى مريضين شابين. الخلايا الجذعية والتنمية 2017 26:6:26، 391-393
[17] رازافي، شاهناز وآخرون. "عوامل التغذية العصبية وتأثيراتها في علاج التصلب المتعدد." متقدم بحوث الطب الحيوي 4 (2015): 53. شركة بي إم سي. الويب. 28 سبتمبر 2018.
[18] J. ك. هوانغ وآخرون تجديد المايلين في التصلب المتعدد: استهداف. الخلايا الجذعية الذاتية المنشأ، الجمعية الأمريكية للعلاجات العصبية التجريبية، 2011
[19] تي لوباتينا وآخرون. (2011) تحفز الخلايا الجذعية المشتقة من الدهون المشتقة من الخلايا الجذعية المشتقة من الدهون تجديد الأعصاب المحيطية: يعزز BDNF الذي تفرزه هذه الخلايا شفاء الأعصاب ونمو المحاور العصبية دي نوفو. PLoS ONE 6(3): e178991
[20] S. سيغو وآخرون، الخلايا التجددية المشتقة من الدهون غير المزروعة تعزز تجديد الأعصاب الطرفية، مجلة علوم تقويم العظام، المجلد 18، العدد 1، 2013، الصفحات 145-151
[21] شو وآخرون عامل التغذية العصبية المشتق من الدماغ يقلل من الالتهاب وموت الخلايا المبرمج في التهاب السحايا العقدي التجريبي بالمكورات الرئوية مجلة الالتهاب العصبي (2017) 14:156
[22] O'Reilly ML وTom VJ (2020) نظام المناعة العصبية كقوة دافعة للمرونة بعد إصابة الجهاز العصبي المركزي. Front. Cell. Neurosci. 14:187.
[23] Blaszkiewicz, M., Wood, E., Koizar, S. et al.. مشاركة الخلايا المناعية العصبية في التعصيب الشحمي. مول ميد 26, 126 (2020)
[24] بيانات داخلية غير منشورة لشركة لوريم سايتوري إنك




 يعد إنجاز ألكسندر تافهًا مقارنةً بفك الشبكة المعقدة من التشابكات التي تنطوي عليها رعاية المرضى الذين لا يملكون خيارًا. هذه المعضلة أكثر تعقيدًا مما قد يبدو للوهلة الأولى.
يعد إنجاز ألكسندر تافهًا مقارنةً بفك الشبكة المعقدة من التشابكات التي تنطوي عليها رعاية المرضى الذين لا يملكون خيارًا. هذه المعضلة أكثر تعقيدًا مما قد يبدو للوهلة الأولى.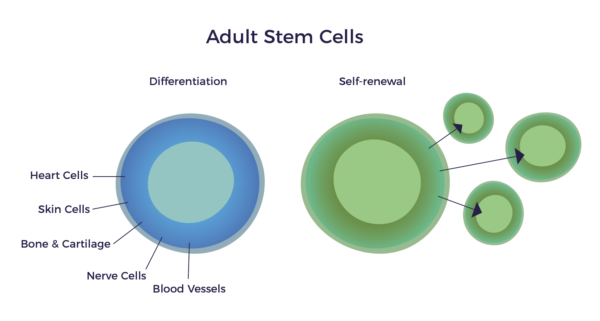
 وكدليل على رؤية الدكتور كابلان وأبحاثه، وفقًا لـ
وكدليل على رؤية الدكتور كابلان وأبحاثه، وفقًا لـ 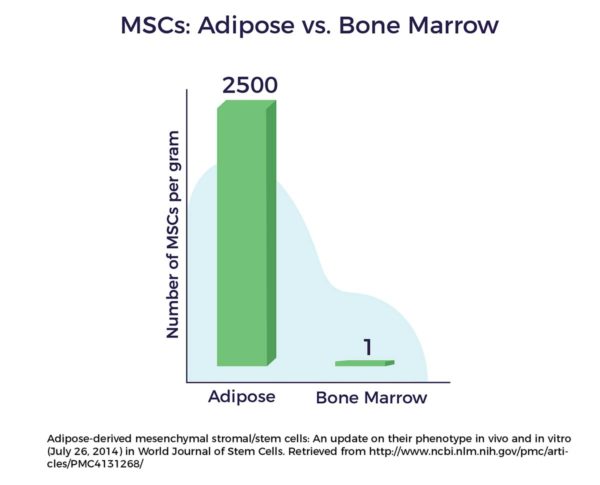
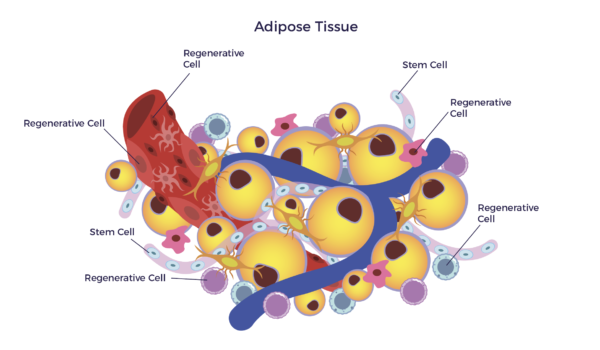 بعبارة أخرى، يوجد مزيج من الخلايا الجذعية والخلايا المتجددة الأخرى في دهوننا. عند الدرجة السريرية، يُطلق على هذا المزيج المتنوع من الخلايا اسم Aثنائي البوصة-Dمشتق Rالتوليد C(ADRCs).
بعبارة أخرى، يوجد مزيج من الخلايا الجذعية والخلايا المتجددة الأخرى في دهوننا. عند الدرجة السريرية، يُطلق على هذا المزيج المتنوع من الخلايا اسم Aثنائي البوصة-Dمشتق Rالتوليد C(ADRCs).