Il existe de nombreuses sources de cellules souches, qui ne sont pas toutes égales. Chez AMBROSE, après avoir examiné ces différentes sources et leurs fonctions, nous nous intéressons aux cellules souches adultes présentes dans le tissu adipeux (graisse).
Les cellules souches et régénératives dérivées de l'adipeuse (ADRC) sont scientifiquement validées comme étant plus accessibles, plus abondantes et plus puissantes que les populations de cellules souches provenant de la moelle osseuse et du sang du cordon ombilical. Elles présentent également un mélange avantageux de types de cellules pour sauver, réparer et régénérer les tissus endommagés, les organes et les systèmes - y compris les systèmes vasculaire, immunitaire, autonome et endocrinien (hormones) - de notre corps. En outre, les facteurs de déclin du rendement et de la puissance liés à l'âge que l'on trouve dans la moelle osseuse ne sont pas observés dans les ADRCS. [1] [2] [3]
Qu'est-ce qu'une cellule souche ?
Le terme cellule souche est apparue pour la première fois dans la littérature scientifique il y a environ 150 ans dans les travaux de l'éminent biologiste allemand Ernst Haeckel (Haeckel, 1868). Haeckel, l'un des principaux partisans de la théorie de l'évolution de Darwin, a dessiné un certain nombre d'arbres ramifiés pour représenter l'évolution des organismes par descendance à partir d'ancêtres communs et a appelé ces arbres "Stammba ̈ ume" (arbres généalogiques ou "arbres tiges" en allemand). Dans ce contexte, Haeckel a utilisé le terme "Stammzelle" (cellule souche en allemand) pour décrire ces cellules comme les cellules les plus fondamentales de notre corps, à partir desquelles toutes les autres cellules se développent.
Cellules souches embryonnaires
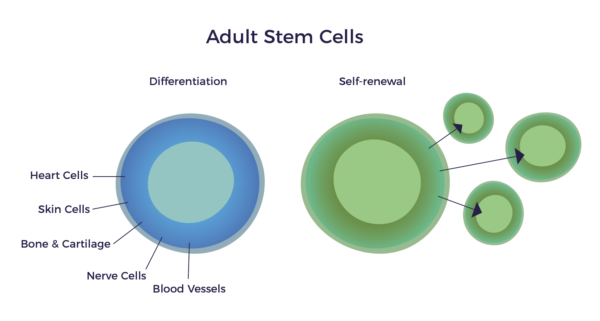
Les cellules souches embryonnaires (CSE) - dont il existe entre 50 et 150 - sont des cellules de développement, ce qui signifie qu'elles se transforment en toutes les lignées cellulaires de notre corps et que ces cellules se répliquent. Elles sont appelées "cellules souches totipotentes", étant les seules cellules capables de donner naissance à tous les types de cellules nécessaires au développement d'un embryon en un corps entièrement formé.
Les CSE peuvent se transformer en chacun des plus de 200 types de cellules du corps adulte lorsqu'elles reçoivent une stimulation suffisante et nécessaire pour un type de cellule spécifique, mais leur utilisation suscite des préoccupations d'ordre éthique et médical. C'est pourquoi elles n'ont fait l'objet que d'un petit nombre d'essais sur l'homme et leur utilisation est illégale dans presque tous les pays développés, y compris les États-Unis.
Cellules souches adultes
- Cellules souches hématopoïétiques - Cellules souches formant les cellules sanguines que l'on trouve dans la moelle osseuse, le tissu du cordon ombilical et le sang.
- Cellules souches mésenchymateuses (CSM) - Cellules souches réparatrices présentes dans tous les tissus de l'organisme, en particulier dans la graisse.
Le terme "cellule souche adulte" est source de confusion, car il s'agit des cellules que nous possédons à la naissance. Les adultes et les enfants possèdent les mêmes cellules souches "adultes". Par conséquent, un nom plus précis et plus descriptif pour ces cellules pourrait être "cellules de réparation", car c'est leur fonction dans un corps pleinement développé. Les cellules souches adultes ne font pas pousser un nouveau cœur, un nouveau cerveau ou de nouveaux os ; elles ont pour but de maintenir ce que nous avons en bon état.
L'histoire de la recherche sur les cellules souches adultes a commencé dans les années 1950, lorsque les chercheurs ont découvert que la moelle osseuse contenait au moins deux types de cellules souches. La première population, appelée cellules souches hématopoïétiques (CSH), forme tous les types de cellules sanguines de l'organisme. Les CSH représentent environ 99,9% des cellules souches de la moelle osseuse et, comme il s'agit de cellules souches formant le sang, elles sont utilisées pour traiter les cancers du sang. Les cellules souches du sang du cordon ombilical sont également constituées en quasi-totalité de CSH et leur utilisation a également été approuvée pour le traitement des cancers du sang.[4] Le tissu du cordon ombilical contient des cellules souches, mais comme elles sont peu nombreuses par gramme, il est nécessaire de les cultiver.
La deuxième population présente dans la moelle osseuse est celle des cellules souches mésenchymateuses (CSM).
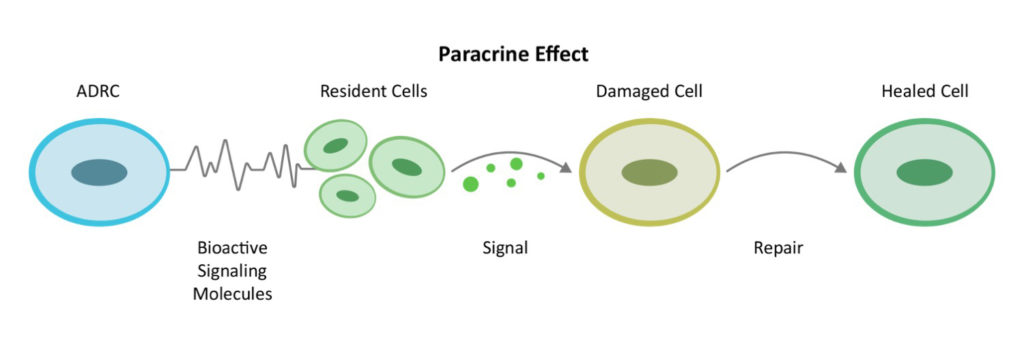
L'origine du concept de cellule souche "mésenchymateuse" remonte aux expériences pionnières de Tavassoli et Crosby dans les années 1960.[5] En 1991, le professeur Arnold Caplan de la Case-Western University a nommé le MSC. [6] D'après une recherche sur Medline, il existe aujourd'hui plus de 49 000 articles publiés sur les CSM et celles-ci ont été utilisées dans plus de 700 essais cliniques. En 2016, le Dr Caplan, dans Les CSM : les sentinelles et les gardiens de la sécurité en cas de blessure[7] a proposé de rebaptiser les cellules souches mésenchymateuses "cellules de signalisation médicinale" en raison de leur fonction de réparation par la communication de cellule à cellule ou "effet paracrine".
 Les CSM sont des cellules souches non hématopoïétiques présentes dans tous les tissus de notre corps. Elles représentent une rare proportion de la population de la moelle osseuse et peuvent se différencier en cellules osseuses, cartilagineuses et adipeuses. Les premières recherches sur les cellules souches adultes se sont concentrées sur la moelle osseuse, mais un problème majeur s'est posé : La quantité et la puissance des cellules souches de la moelle osseuse diminuent avec l'âge et en présence de maladies chroniques.
Les CSM sont des cellules souches non hématopoïétiques présentes dans tous les tissus de notre corps. Elles représentent une rare proportion de la population de la moelle osseuse et peuvent se différencier en cellules osseuses, cartilagineuses et adipeuses. Les premières recherches sur les cellules souches adultes se sont concentrées sur la moelle osseuse, mais un problème majeur s'est posé : La quantité et la puissance des cellules souches de la moelle osseuse diminuent avec l'âge et en présence de maladies chroniques.
Avantages du tissu adipeux
Les graisses sont plus nombreuses qu'il n'y paraît. Alors que de nombreux chercheurs se concentrent uniquement sur les CSM présentes dans la moelle osseuse, la graisse, le cordon ombilical, le placenta, la pulpe dentaire et ainsi de suite, dans la graisse, elles ne sont pas sans rappeler le chanteur principal d'un groupe dont la musique est enrichie et améliorée par les choristes et les autres musiciens. Il existe dans la graisse de nombreux autres types de cellules qui travaillent ensemble et que nous appelons "cellules régénératrices".
Le tissu adipeux fonctionne comme un réservoir protégé de cellules souches et régénératrices tout au long de la vie. Les études utilisant des cellules mononucléaires de la moelle osseuse (BMNC) pour la moelle osseuse ont constaté une chute brutale de l'efficacité après l'âge de 62 ans.[8]
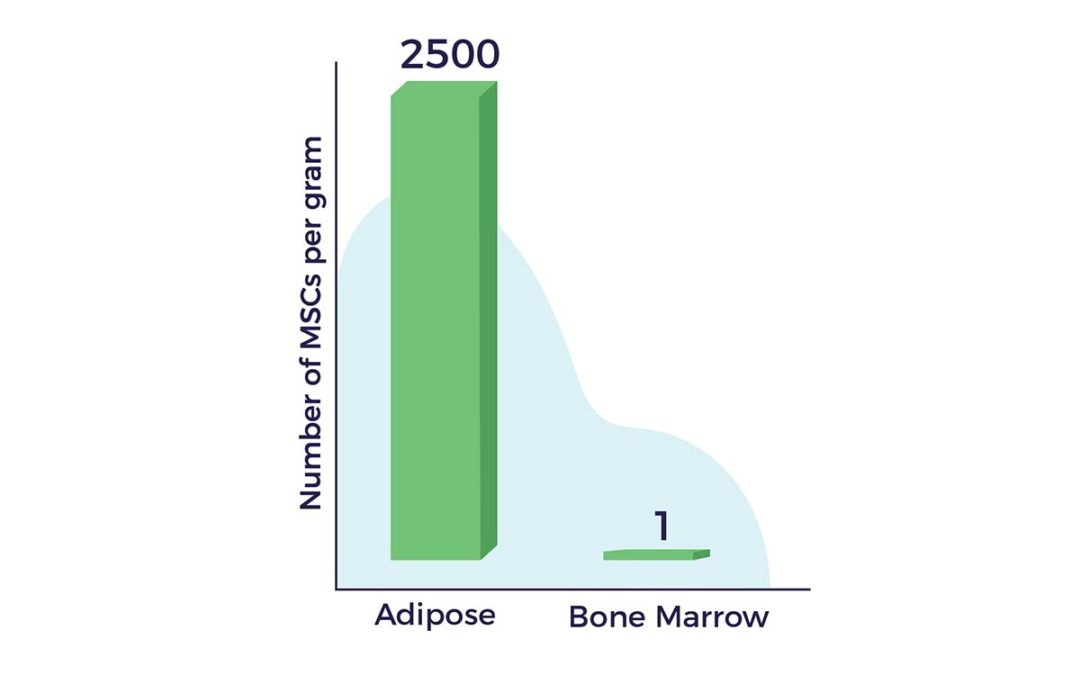
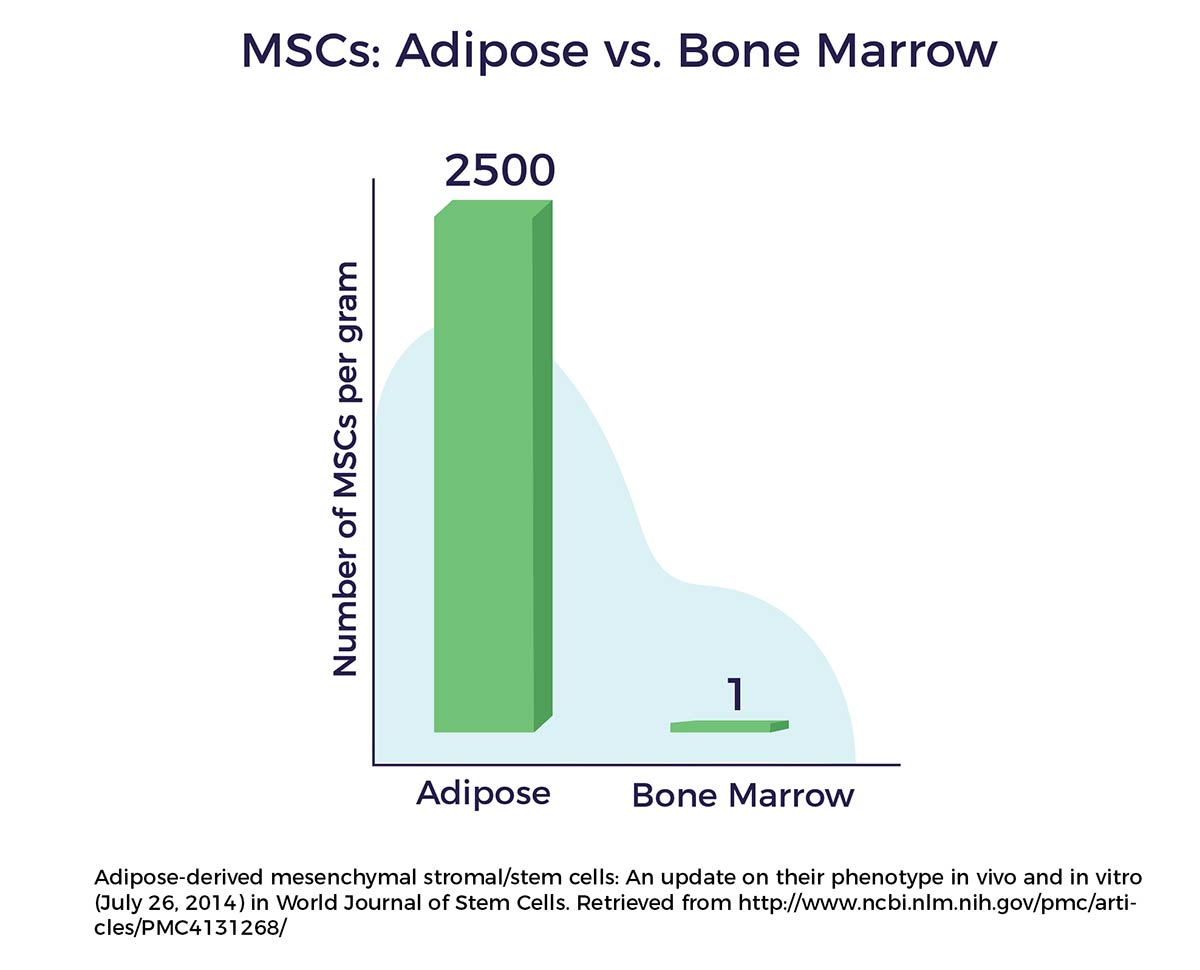
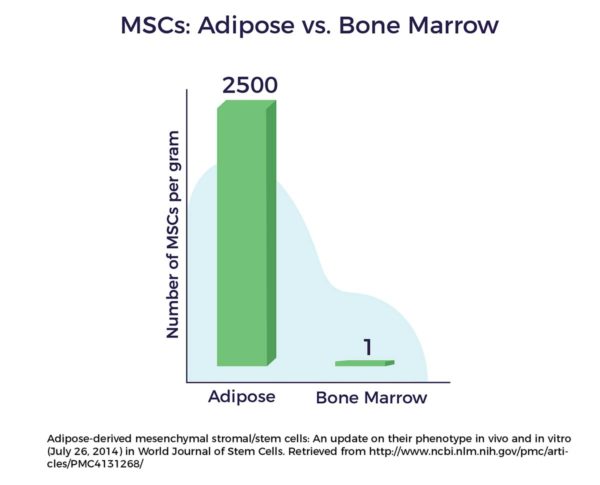
Un autre avantage de la graisse comme source de cellules réside dans le fait qu'il y a jusqu'à 2 500 fois plus de CSM dans un gramme de tissu adipeux que dans un gramme de moelle osseuse. [9]
Les cellules régénératives dérivées de la graisse ont été découvertes pour la première fois en 1964 par Martin Rodbell qui, à l'aide d'une enzyme et d'une centrifugeuse, a réussi à libérer une population mixte de cellules du tissu adipeux d'une souris. La recherche sur les cellules souches adultes a fait un bond en avant en 2001, lorsque Patricia Zuk PhD, le Dr Marc Hedrick et d'autres personnes travaillant dans les laboratoires de l'UCLA, ont publié un article dans Tissue Engineering sur leur découverte que les cellules souches mésenchymateuses (CSM) résident dans le tissu adipeux et dans le tissu adipeux, et qu'elles sont donc capables de régénérer le tissu adipeux. avec d'autres cellules régénératrices dans notre graisse.[10] Une nouvelle ère de la médecine s'ouvre alors.
Des cellules différentes, des emplois différents
Les cellules souches adultes provenant de différentes sources cellulaires sont utilisées pour différentes indications, notamment certains cancers du sang pour les cellules souches de la moelle osseuse et du cordon ombilical. Les cellules souches de la moelle osseuse se sont révélées plus efficaces dans la thérapie cellulaire orthopédique et cardiaque chez les patients d'âge moyen ou plus jeunes, en raison de la diminution de leur nombre et de leur puissance avec l'âge. À l'inverse, les cellules souches du cordon ombilical sont accessibles, abondantes et puissantes plus tard dans la vie et sont donc les plus prometteuses pour les maladies dégénératives liées à l'âge.